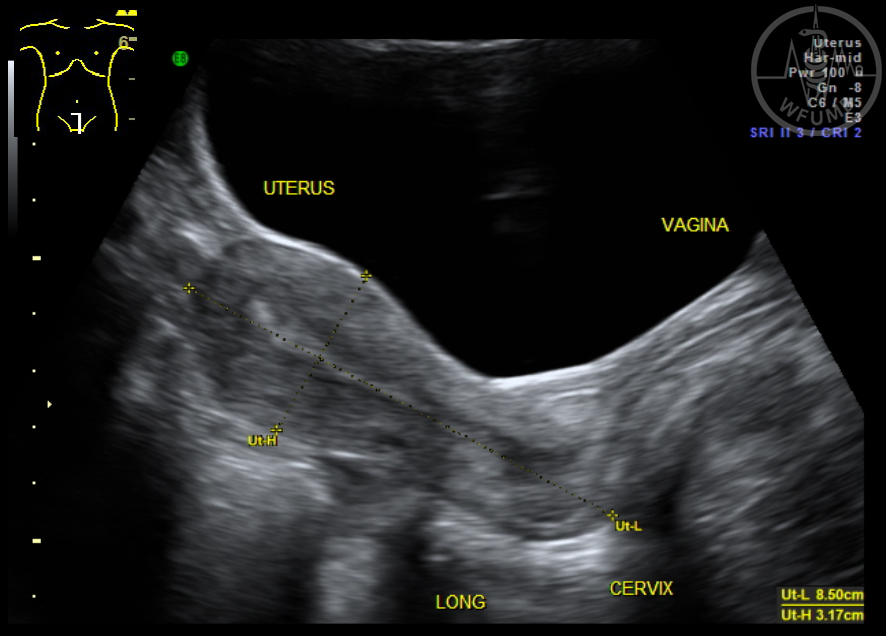
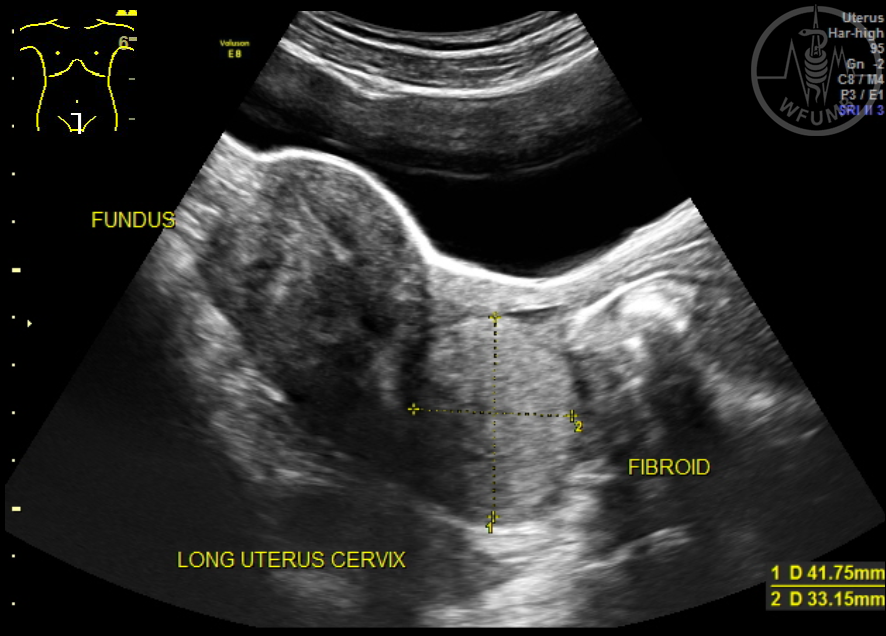
Fig 20.2.1
Anteverted uterus. In the long axis, image the entire length of uterus, cervix and vagina. Measure length & height
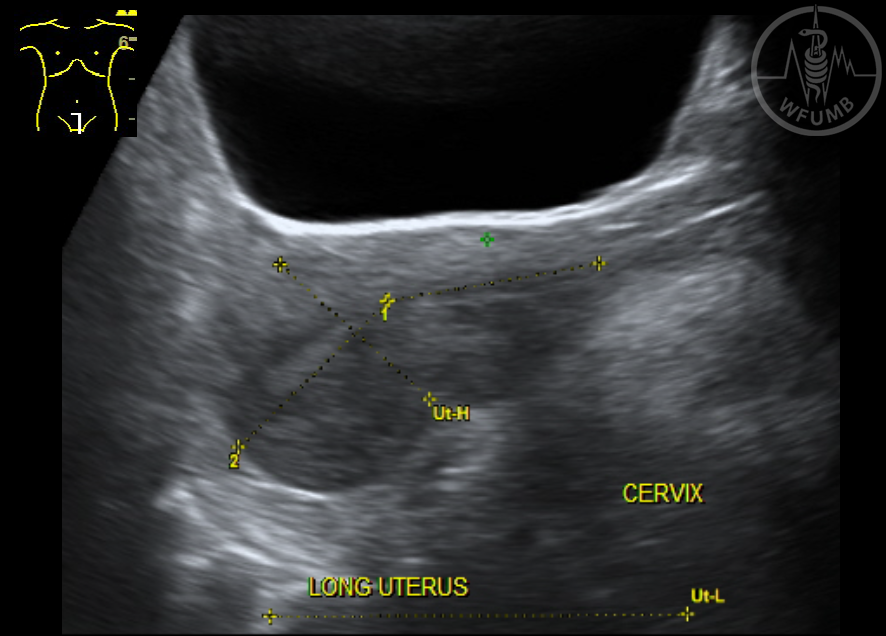
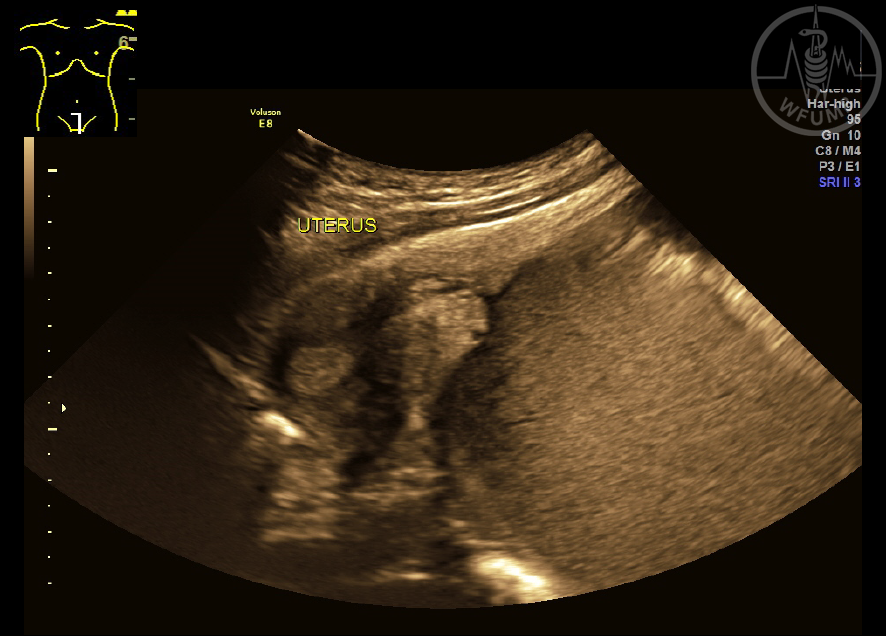
Fig 20.2.2a
Trans-abdominal image of a retroverted uterus. It is tilted posterior which often makes the assessment of the fundus and endometrium more difficult with TA scanning
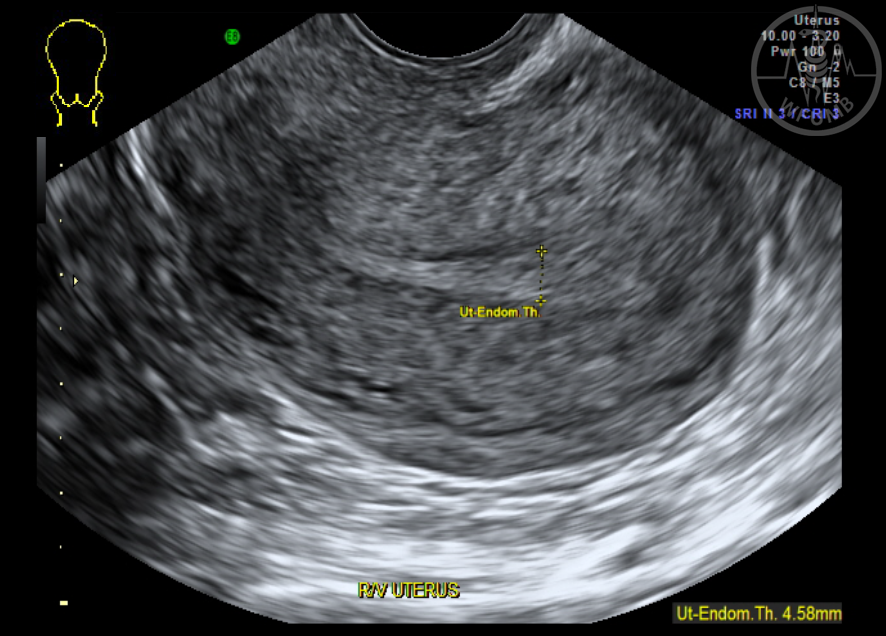
Figure 20.2.2b
TV image of the retroverted uterus and so the uterine fundus is on the right of the screen and the anterior uterine wall appears in the far field of the image
Fig 20.2.3
Midline transverse TA image of the uterus which is deviated to the right of midline. Both ovaries can be clearly seen
Fig 20.2.4a
TV transverse image of a bicornuate uterus. Best imaged in the transverse view, the endometrial cavity is seen to divide as the transducer is moved superiorly. Note the central dip at the fundal region
Fig 20.2.4b
TV transverse image of a uterus didelphys with a gestational sac in the right horn. Best imaged in the transverse view, the uterus is seen to divide into two distinct uteri as the probe is moved towards the fundus
Fig 20.2.4c
TV / 3D transverse image of a didelphys uterus showing the 2 distinct uteri and endometrium
Fig 20.2.5
Haematocolpus - a blood collection in the vaginal cavity. Causes can include an imperforate hymen, a vaginal septum or vaginal atresia
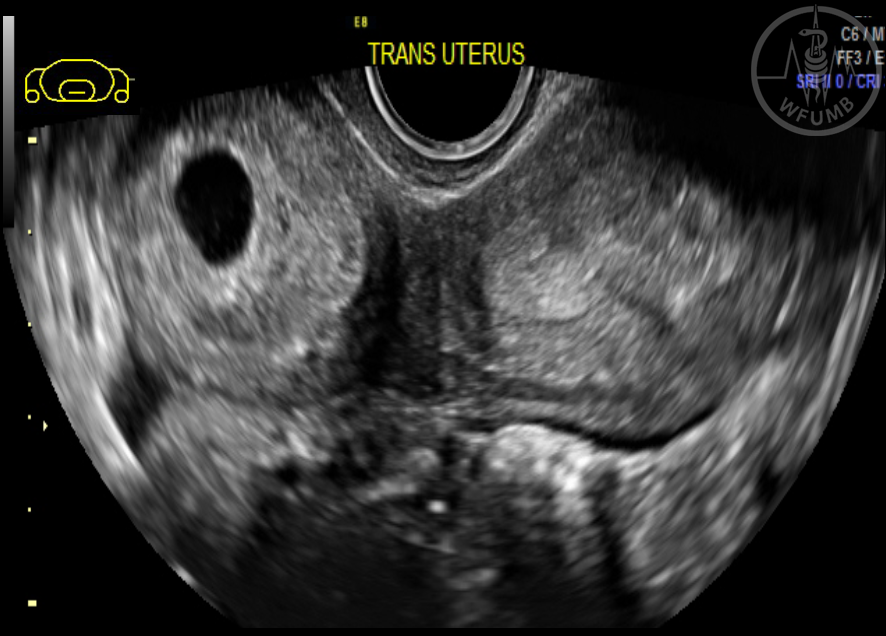
Fig 20.2.6
TV image of intramural fibroids within the anterior aspect of a retroverted uterus
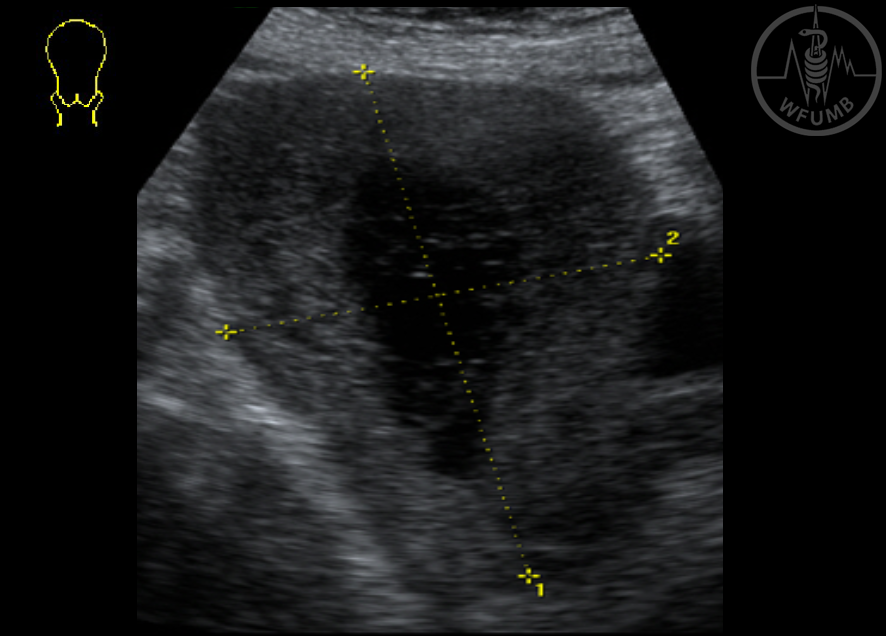
Fig 20.2.7
TV image of a cystic intramural fibroid in the posterior aspect of the uterus. Do not mistake it for a cystic ovary
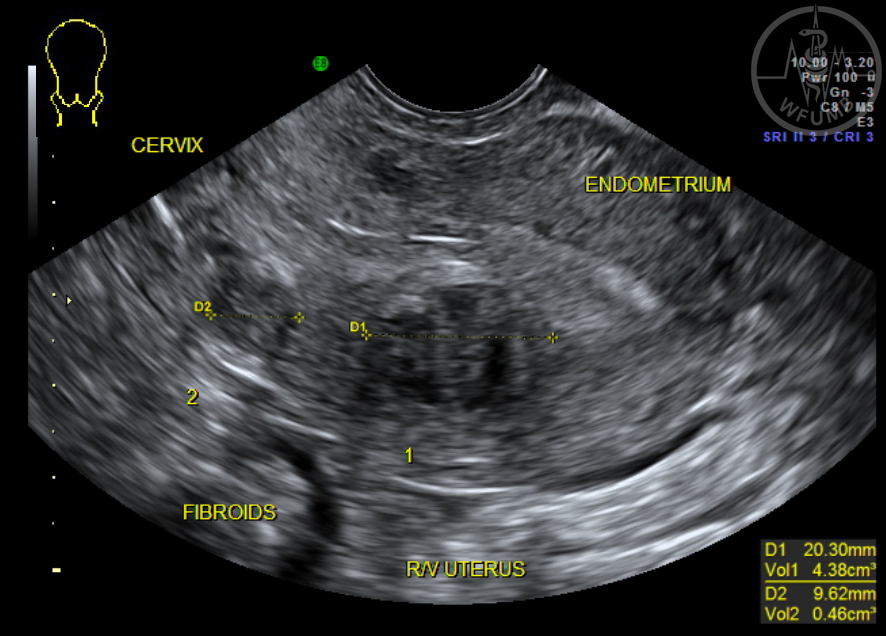
Fig 20.2.8
Cervical fibroid seen in the posterior aspect of the cervical canal
Fig 20.2.9
This TA image shows 3 sub-serosal fibroids projecting from the uterine surface
Fig 20.2.10
TV image of a submucosal fibroid which indents the endometrium. Submucosal fibroid usually cause the most symptoms and it is important to differentiate between those that indent the endometrium versus those that become pedunculated or prolapse into the cervical canal
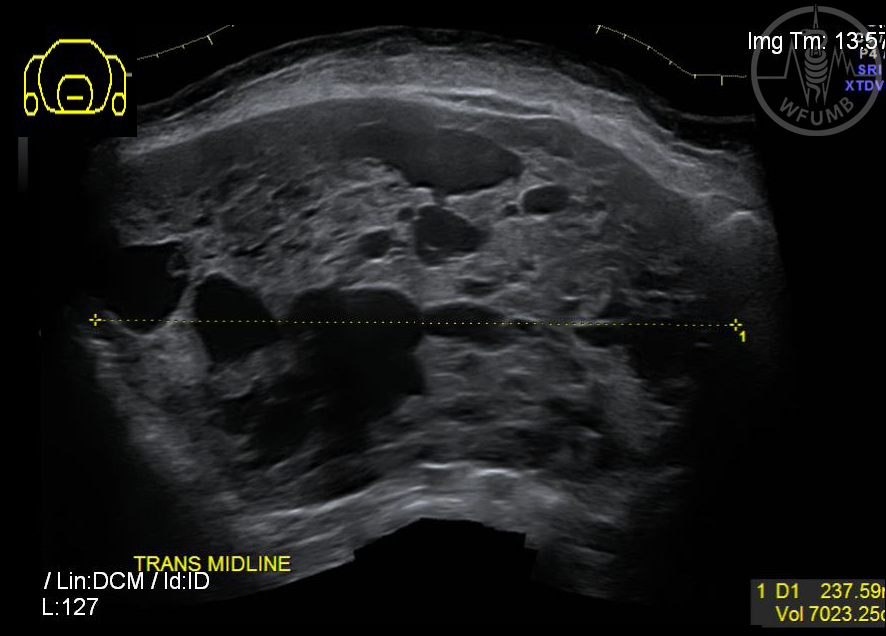
Fig 20.2.11
displays a very large uterine cancer with a volume of over 7000 mls. The patient was 65 and presented with abdominal bloating but no pain
Fig 20.2.12
TA image of the uterus with a 7cm squamous cell carcinoma in a 35 year old who presented with a 3 month history of vaginal bleeding with clots
Fig 20.2.13a
TA image of a uterus with adenomyosis in the anterior myometrium
Fig 20.2.13b
TV image which clearly shows the classic streaking appearance of adenomyosis in the posterior myometrium. Note that the posterior myometrium is much wider than the anterior myometrium
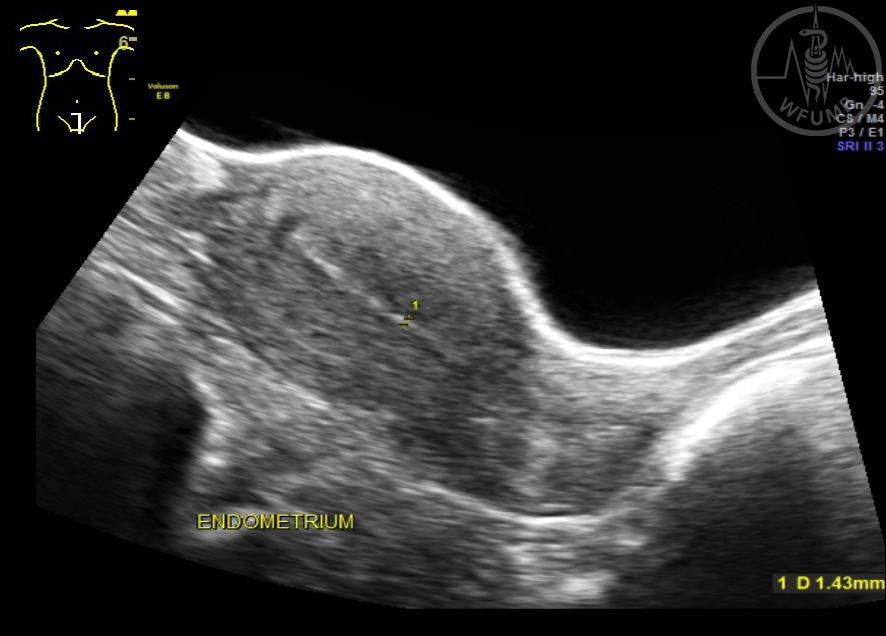
Fig 20.2.14
Demonstrates the menstrual phase (1-4mm) days 1 to 5, a single thin line which is the basal layer of the endometrium
Fig 20.2.15
Proliferative phase (4-10mm). The endometrium appears as a triple line, with the centre line being the basal layer
Fig 20.2.16
Secretory phase
(7-18mm) from day 14, or time of ovulation, onwards, and appears as a thick hyperechoic line which gets thicker approaching menses
Fig 20.2.17
Endometrium with hyperplasia. A thickened endometrium may be caused by adhesions, hyperplasia, polyps, endometrial cancer, very early intrauterine pregnancy, incomplete miscarriage, failed pregnancy, ectopic pregnancy, retained products of conception, trophoblastic disease or hormone replacement therapy
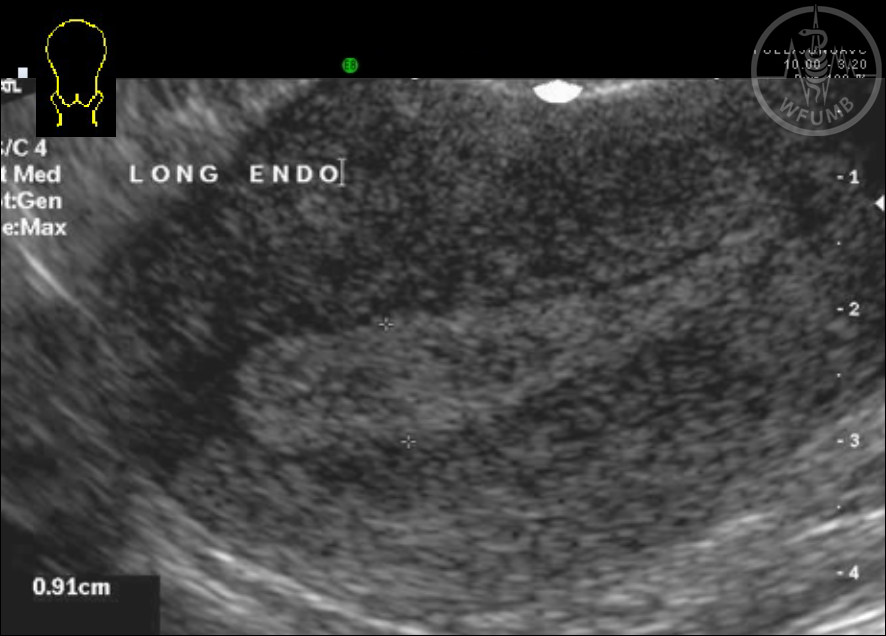
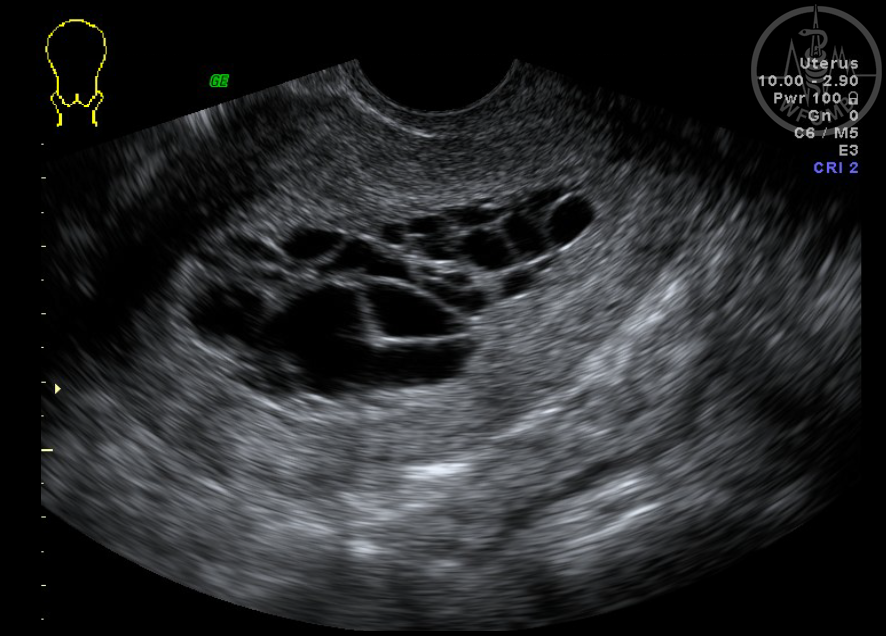
Fig 20.2.18
TV image of cystic hyperplasia of the endometrium. The possible causes include prolonged proliferative phase from chronic anovulation e.g. those with polycystic ovaries or long term oral contraceptive in premenopausal women
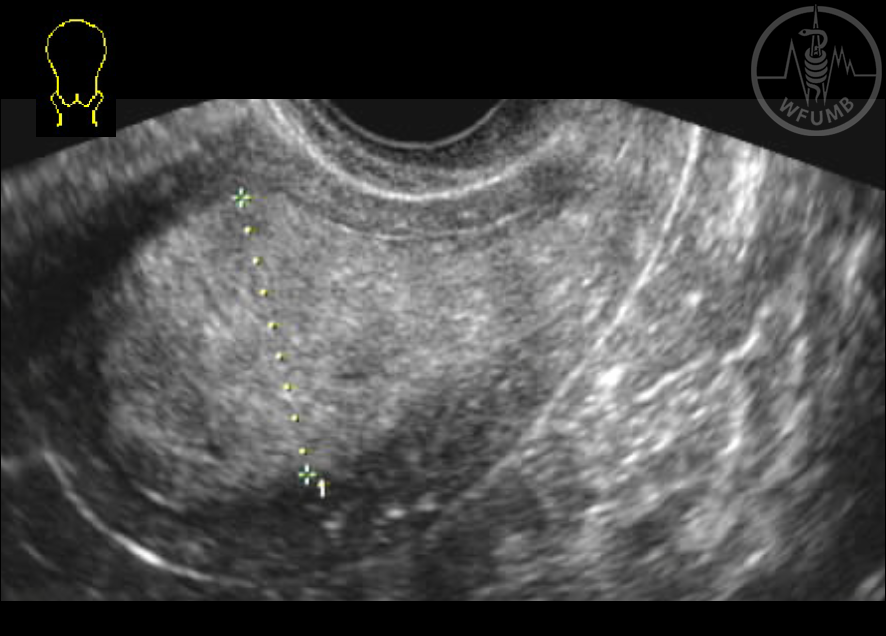
Fig 20.2.19a
Large well defined ovoid mass within the endometrium which could be a polyp or a fibroid
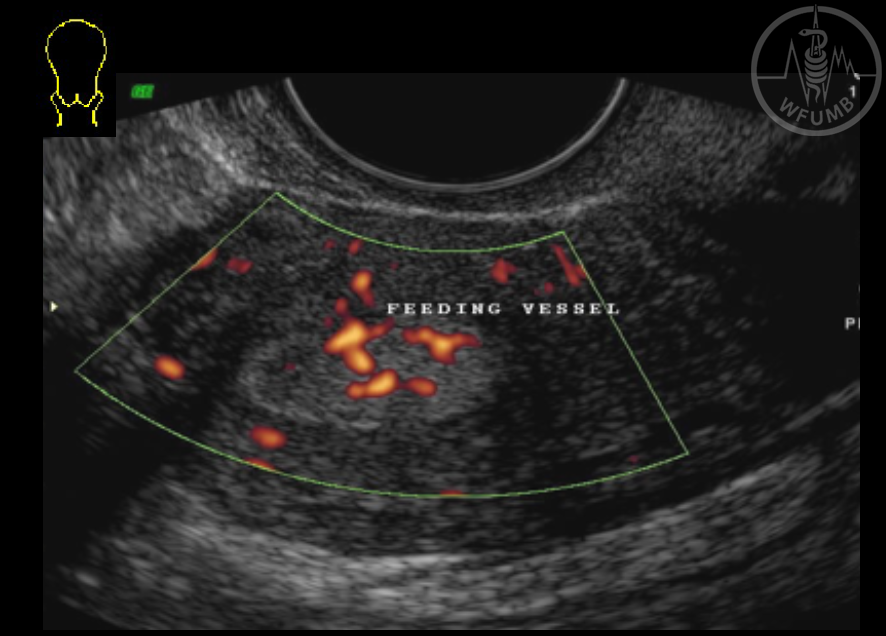
Fig 20.2.19b
Adding colour Doppler (same case as Figure 20.2.19a) shows a feeder vessel which indicates a polyp
Fig 20.2.20
A case of post-partum endometritis
Fig 20.2.21
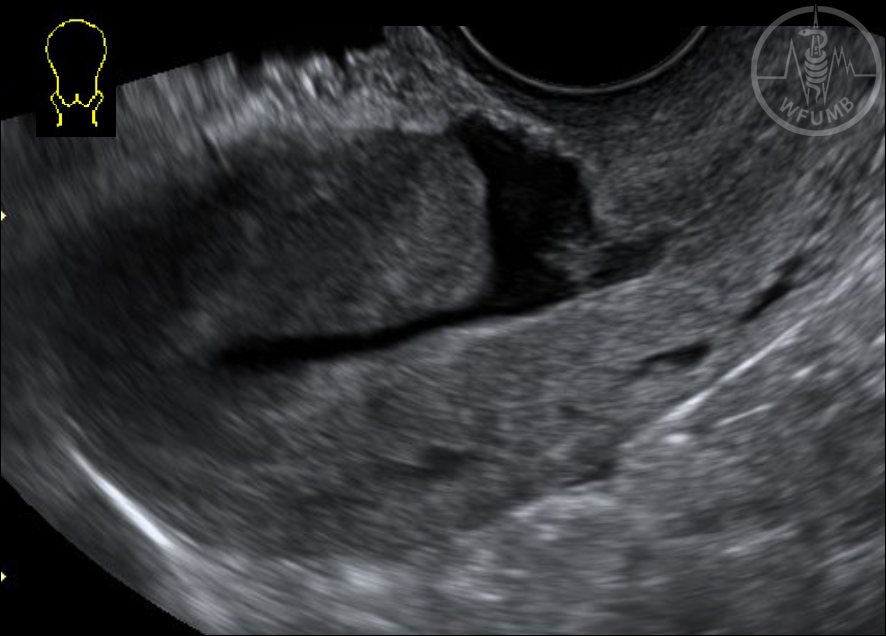
TV image of hematometra where the endometrial cavity is expanded by a blood collection
Fig 20.2.22
shows an ill-defined hyperechoic mass in the endometrium which is an example of retained products of conception
Fig 20.2.23
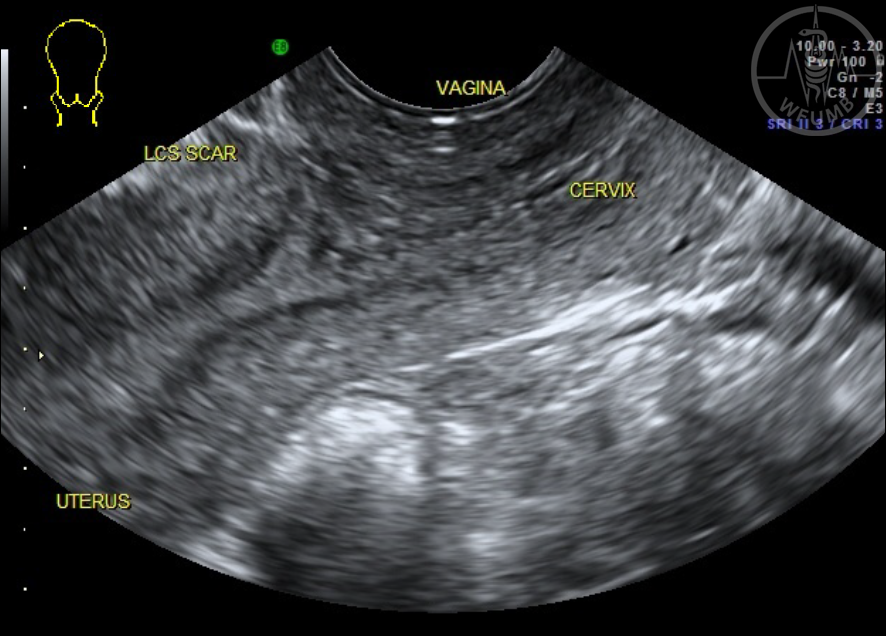
Normal caesarean scar on the lower anterior myometrium of the uterus
Fig 20.2.24
Caesarean section scar defect running from the endometrium to the anterior uterine wall
Fig 20.2.25a
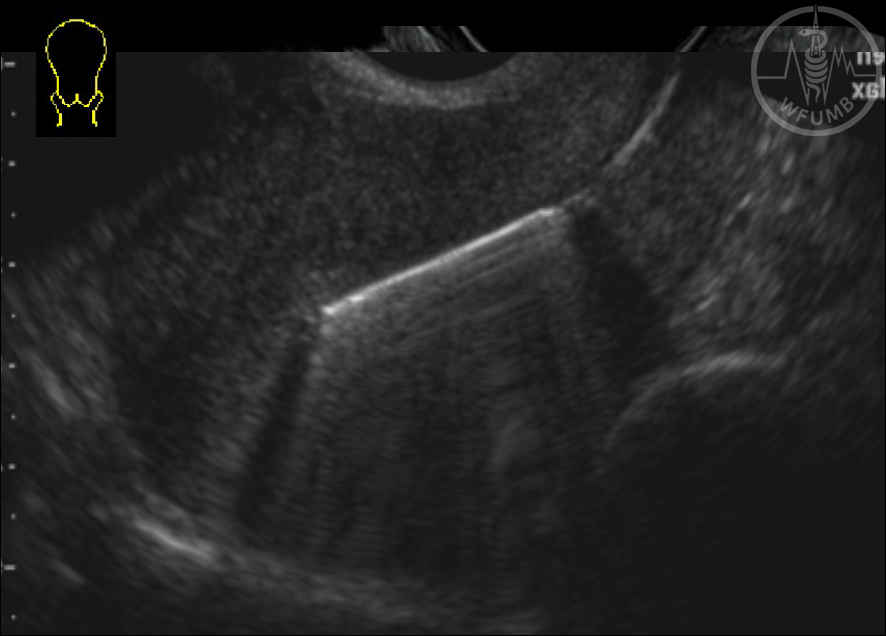
TV image which shows a correctly placed intra uterine contraceptive device (IUCD)
Fig 20.2.26a.
The ovary is usually situated in the ovarian fossa, lateral to the uterus on the posterior surface of the broad ligament, below the fallopian tubes
Fig 20.2.26b.
The ovary is usually situated in the ovarian fossa, medial to the external iliac and anterior to the internal iliac vessels
Fig 20.2.27
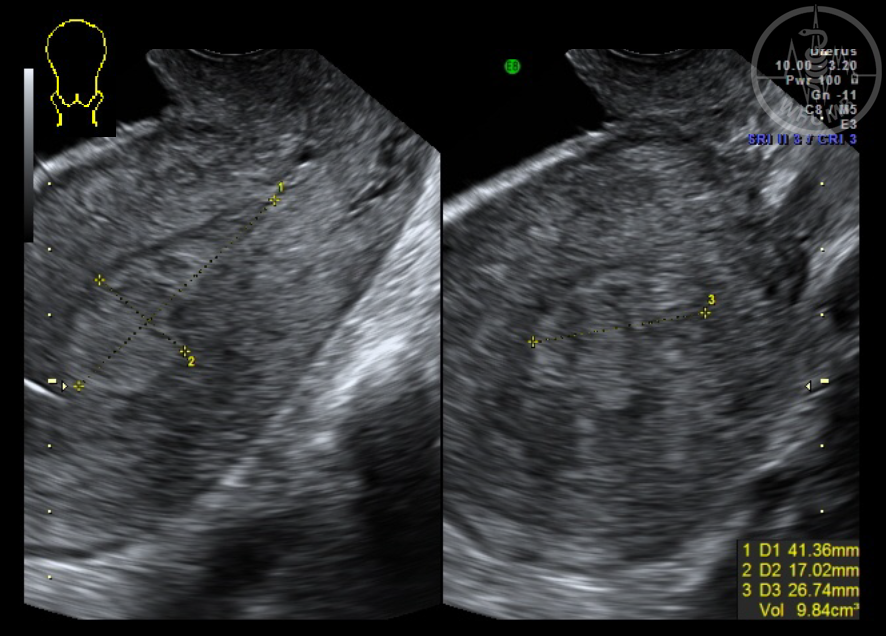
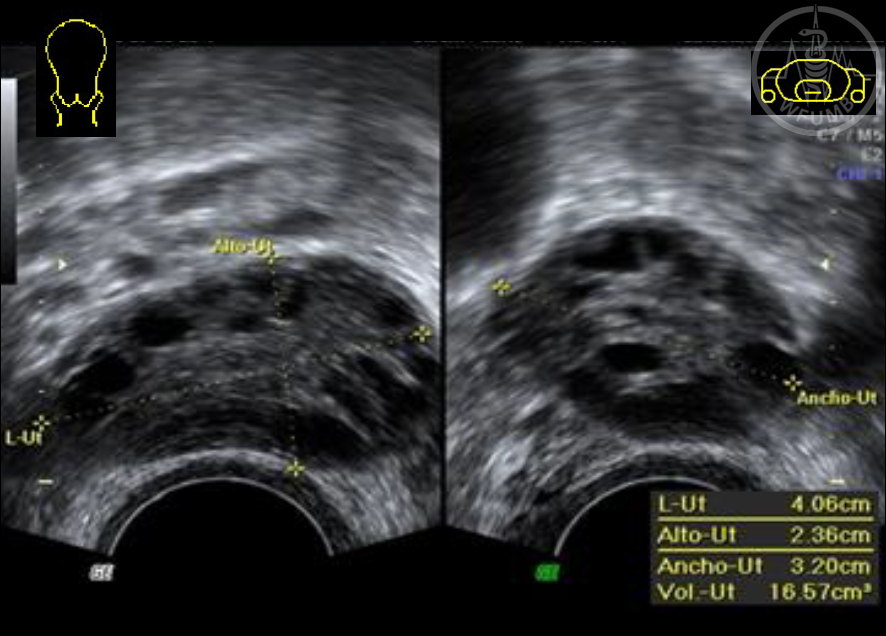
The volume of the ovary is calculated by imaging the ovary in a transverse and sagittal plane and measuring length, height and width, (L x H x W) / 2
Fig 20.2.28
Follicles grow around 2mm per day, with the dominant follicle measuring between 20 – 25 mm at ovulation
Fig 20.2.29
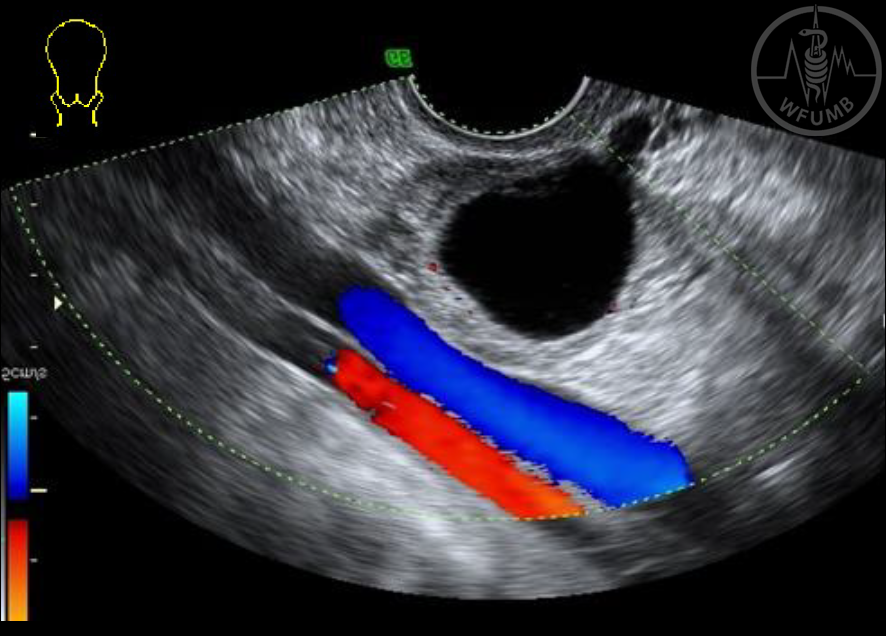
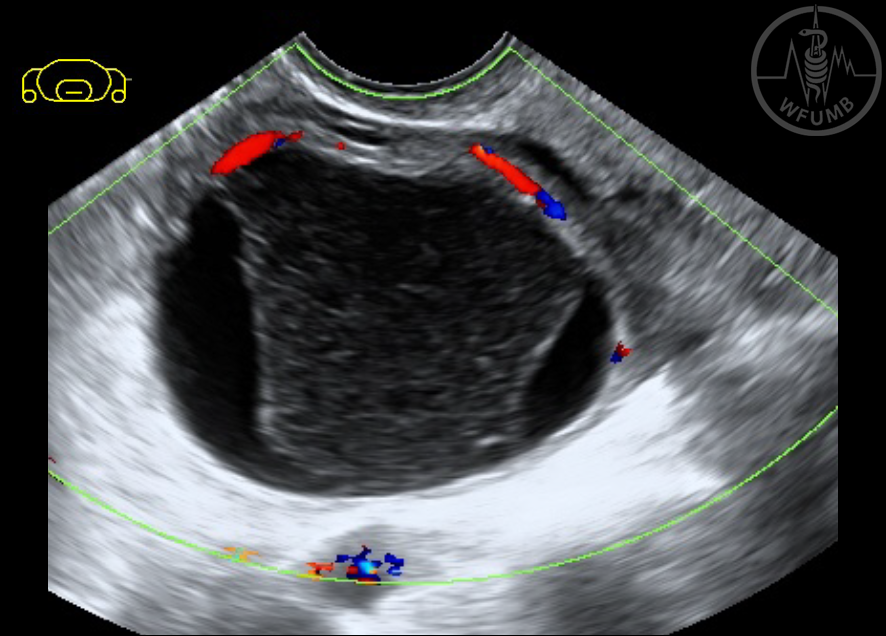
The ultrasound appearance of the corpus luteum can vary from cystic to haemorrhagic.
Colour Doppler imaging may display high vascularity, low-resistance peripheral flow that is often termed the’ ring of fire’
Fig 20.2.30
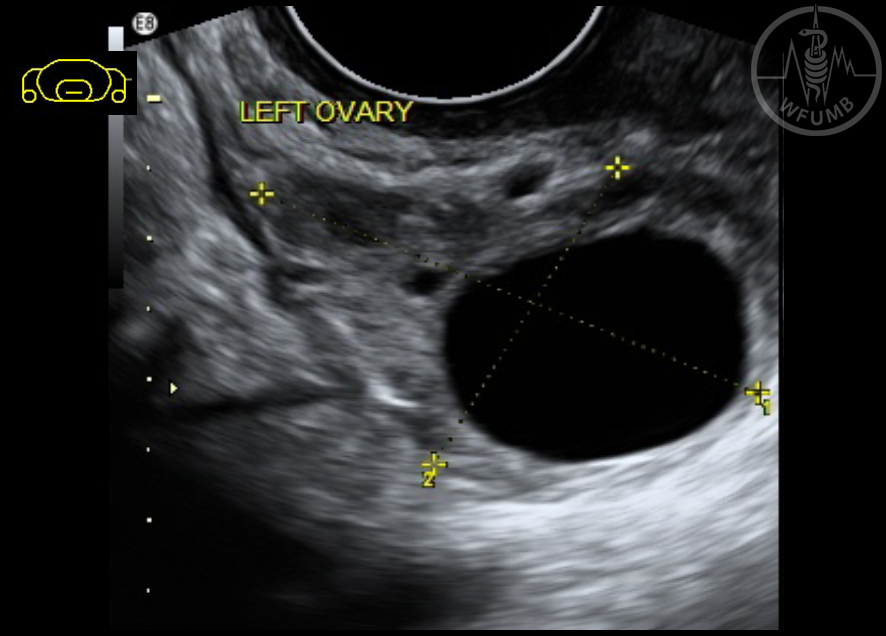
Simple ovarian cysts are anechoic, unilocular, non-septated, thin walled with posterior enhancement
Fig 20.2.31
is a classic image of a haemorrhagic cyst. As the clot retracts it is surrounded by fluid
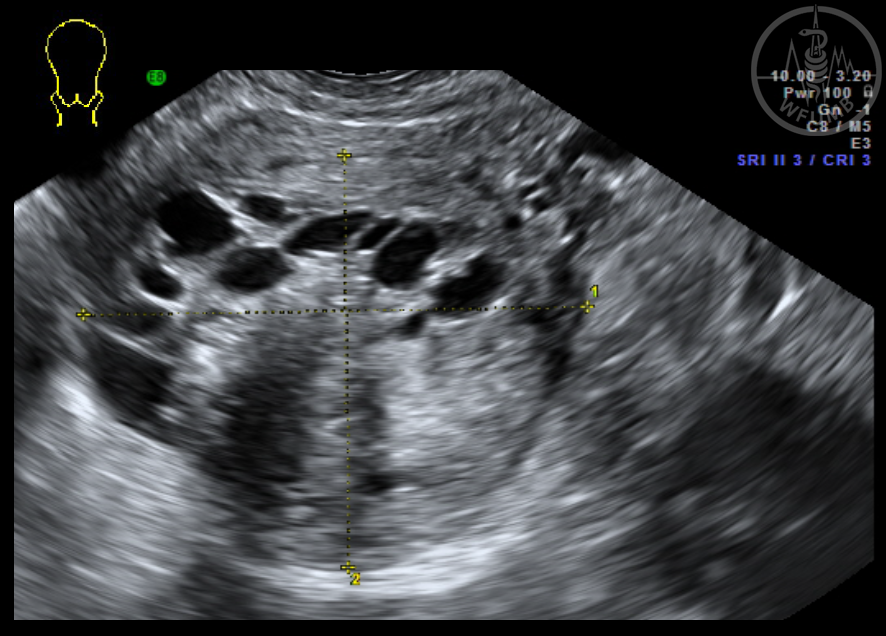
Fig 20.2.32
Typical image of a polycystic ovary
Fig 20.2.33a
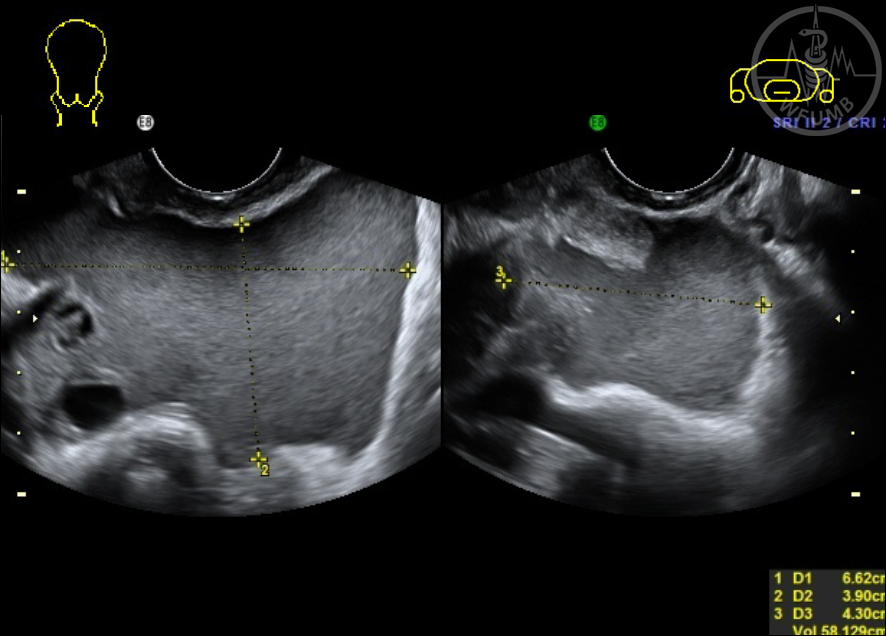
Transverse image of the uterus with bilateral ovarian hypertrophy caused by hyperstimulation from IVF treatment
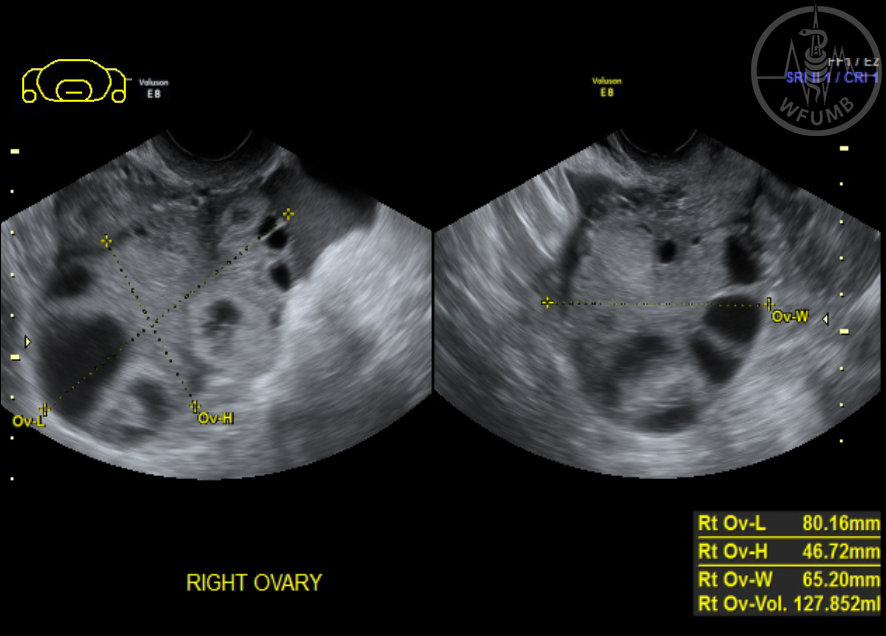
Fig 20.2.33b
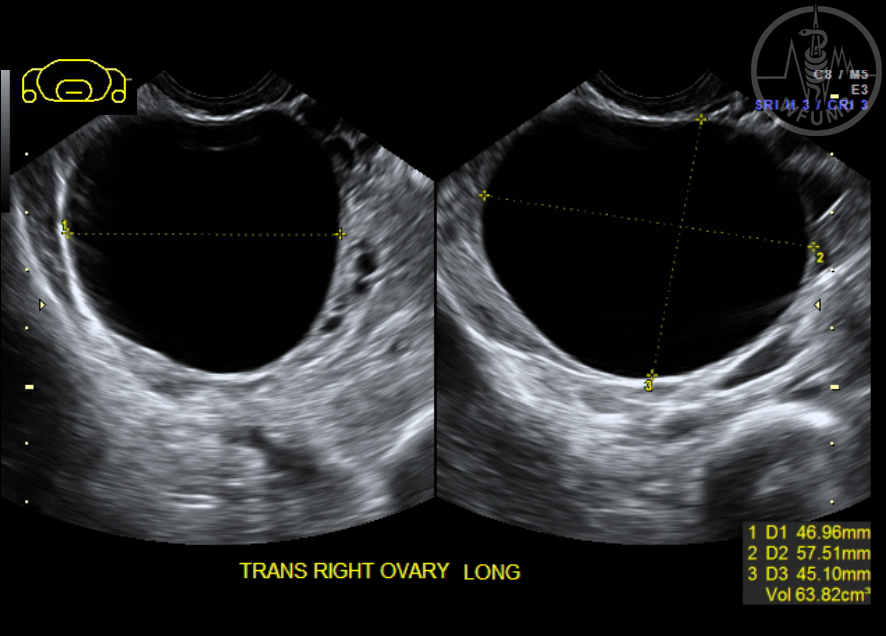
is an overstimulated ovary with a volume of 127mls
Fig 20.2.34a
Typical endometrioma
Fig 20.2.34b Endometrioma with solid content
Fig 20.2.35
A dermoid may be seen as a unilocular cystic mass with in-homogenous content, mural projections or hyperechoic masses
Fig 20.2.36
Large cystadenocarcinoma. Colour is useful to look for vascularity in the solid components
Fig 20.2.37. Particulate matter in fluid in the pouch of Douglas could be blood or pus
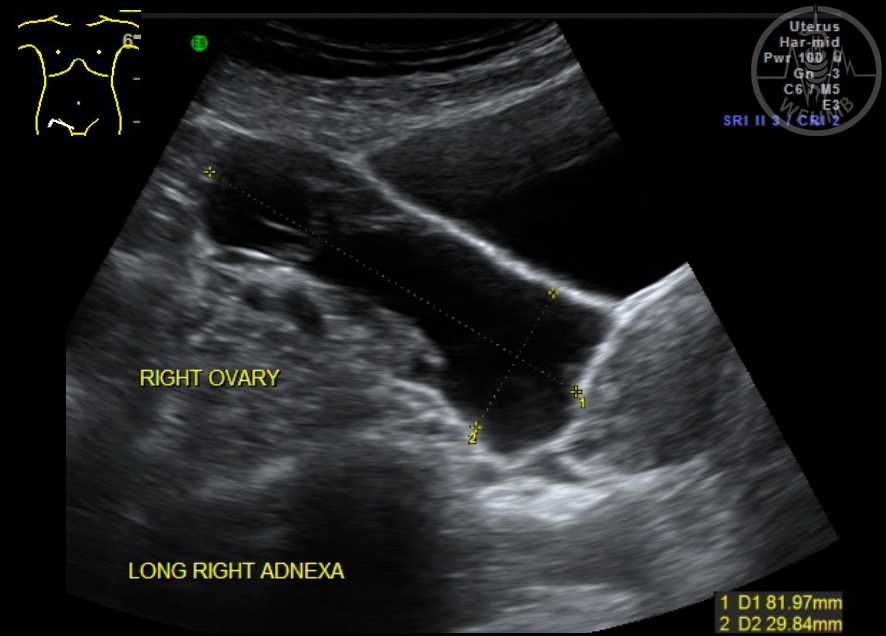
Fig 20.2.38a
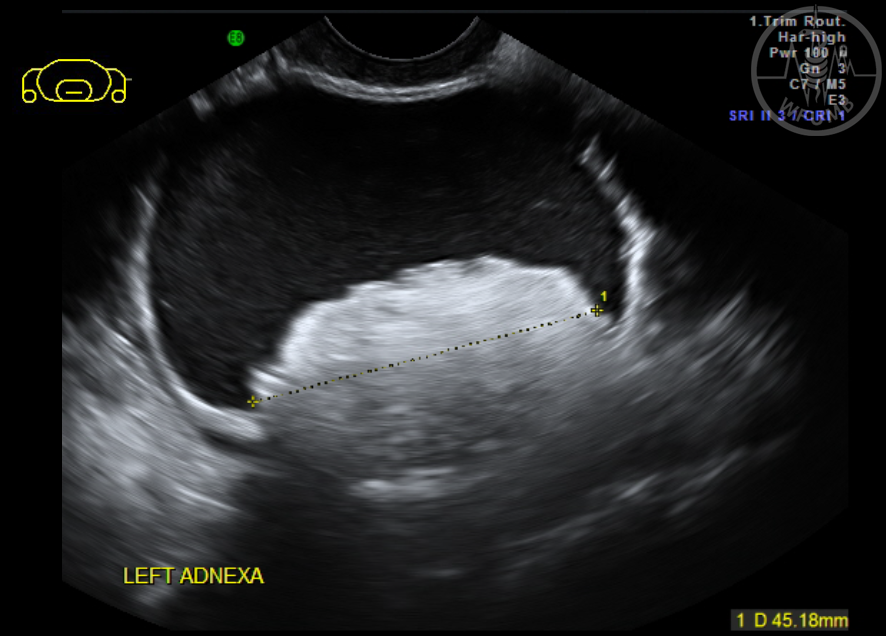
A hydrosalpinx on ultrasound appears as an anechoic tubular structure with incomplete septa (TA scan of a dilated tube adjacent to the right ovary)
Fig 20.2.38b
Pyosalpinx - pus accumulates in the tube and there is a thickened tubal wall associated with acute inflammation
Fig 20.2.39a
Normal bowel – TV view
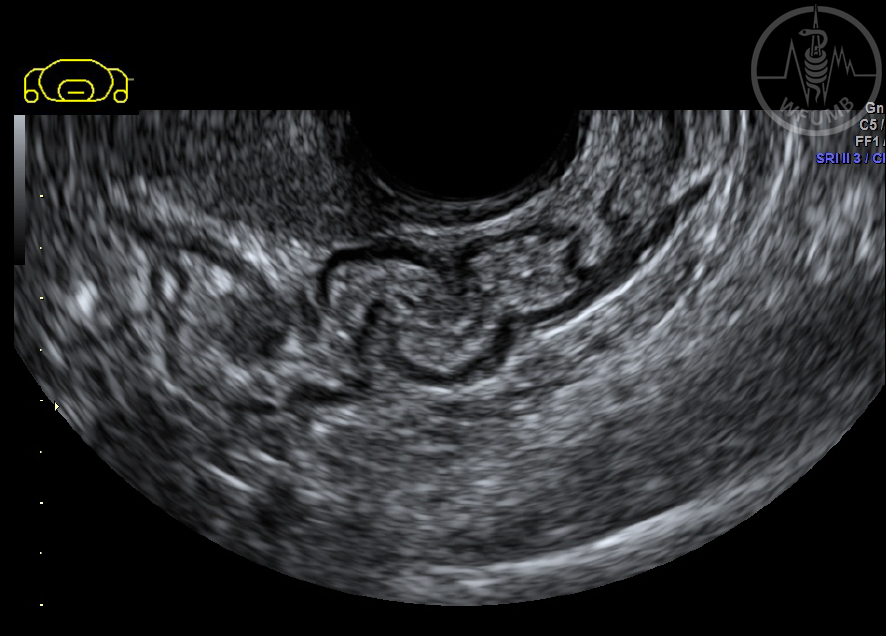
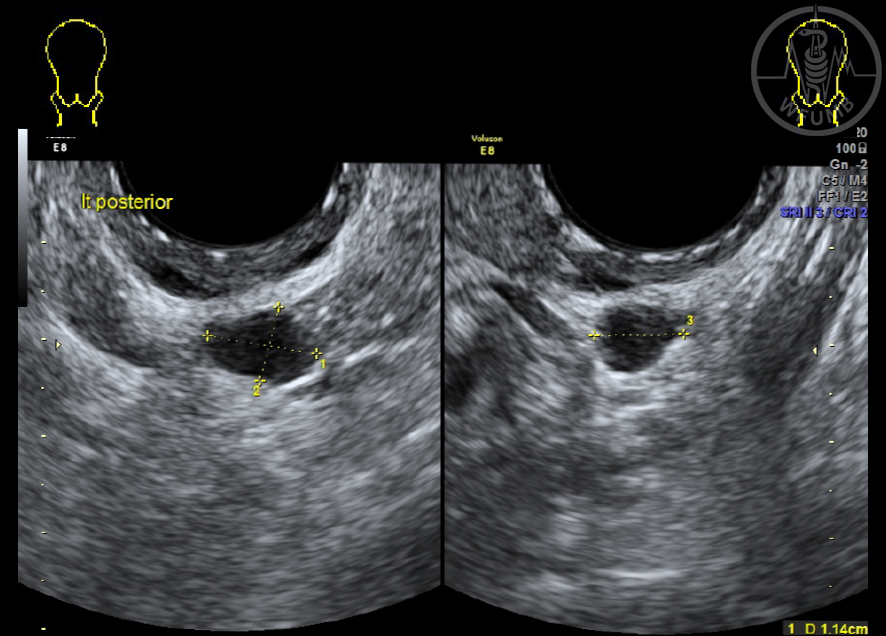
Fig 20.2.39b
Deep infiltrating endometriosis (DIE) (TV view)
Fig 20.2.40.
The uterus is surrounded by fluid from ascites as a result of malignancy (TV view)