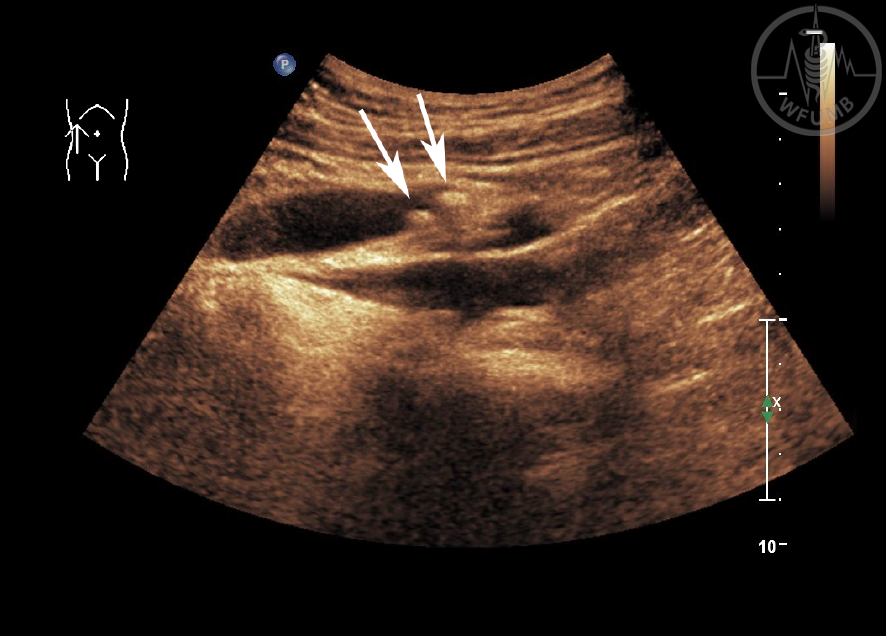
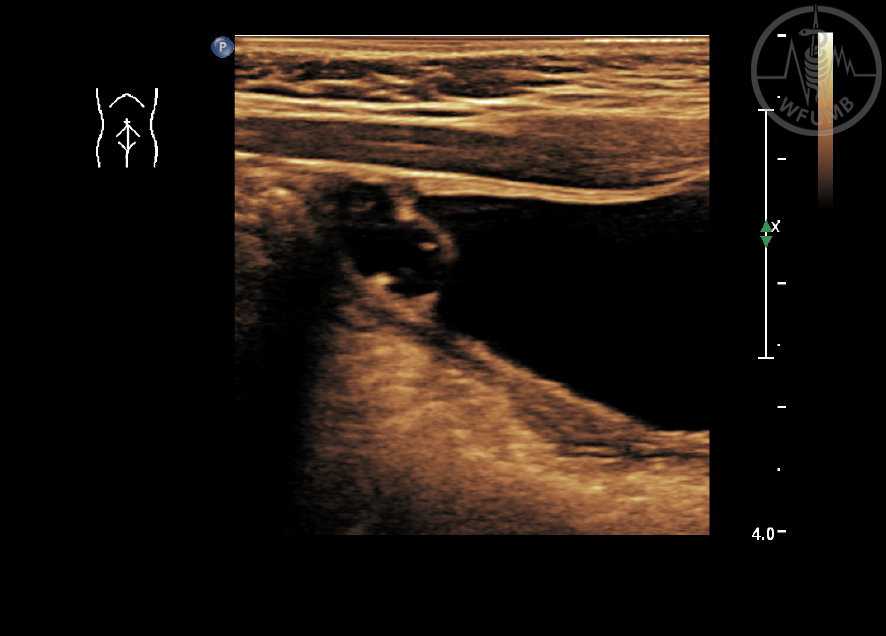
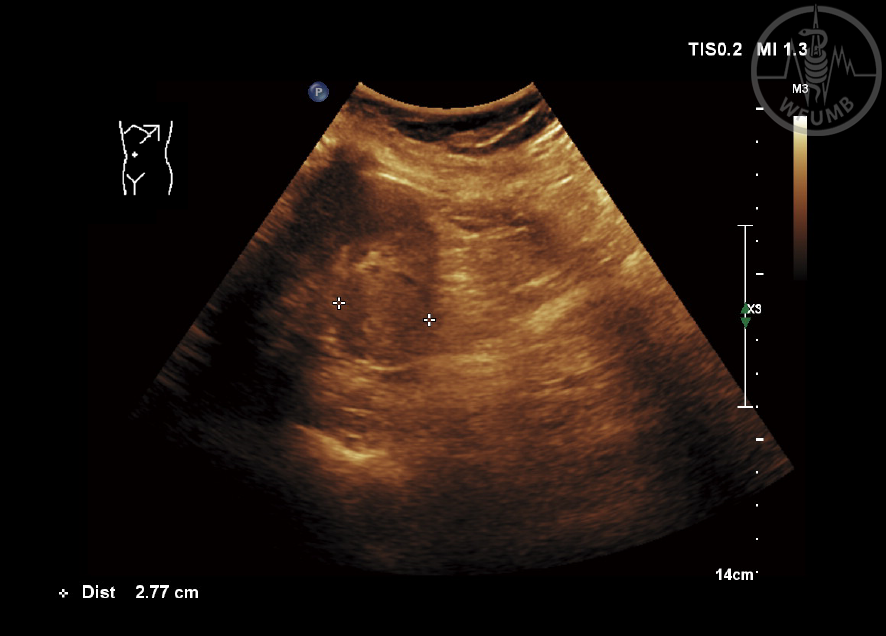
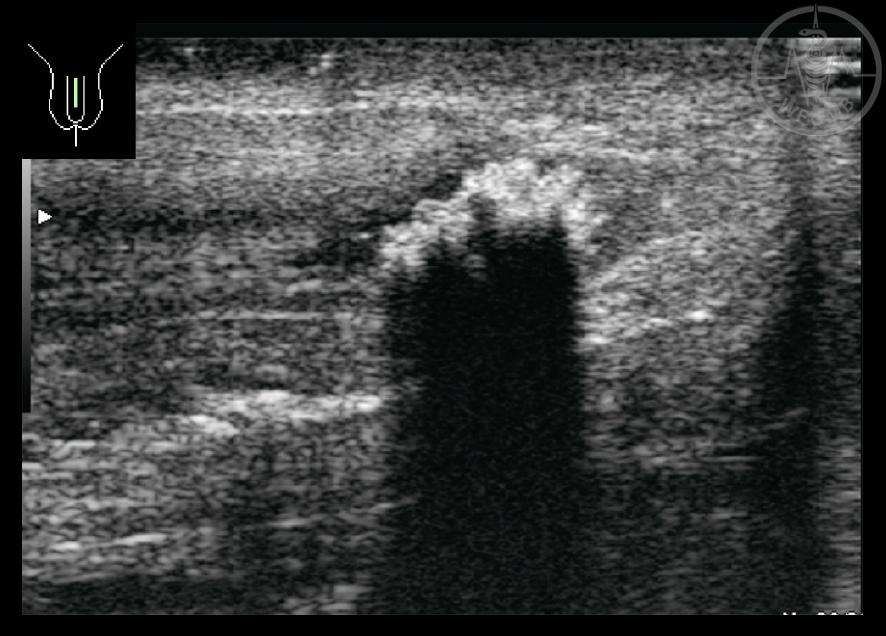
Fig 21.2
Right (ri) ureter longitudinal. Stones (arrows) in region of crossover iliac vessels
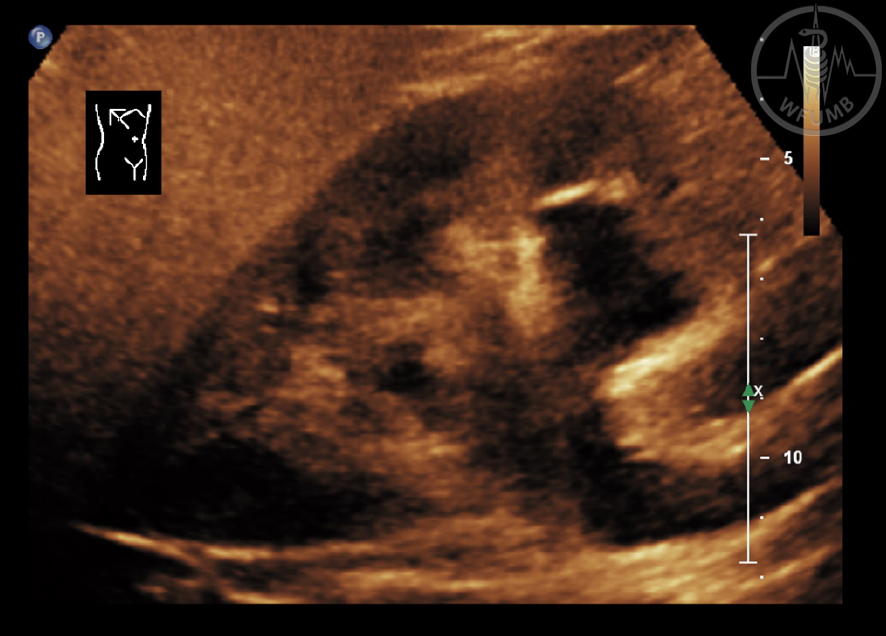
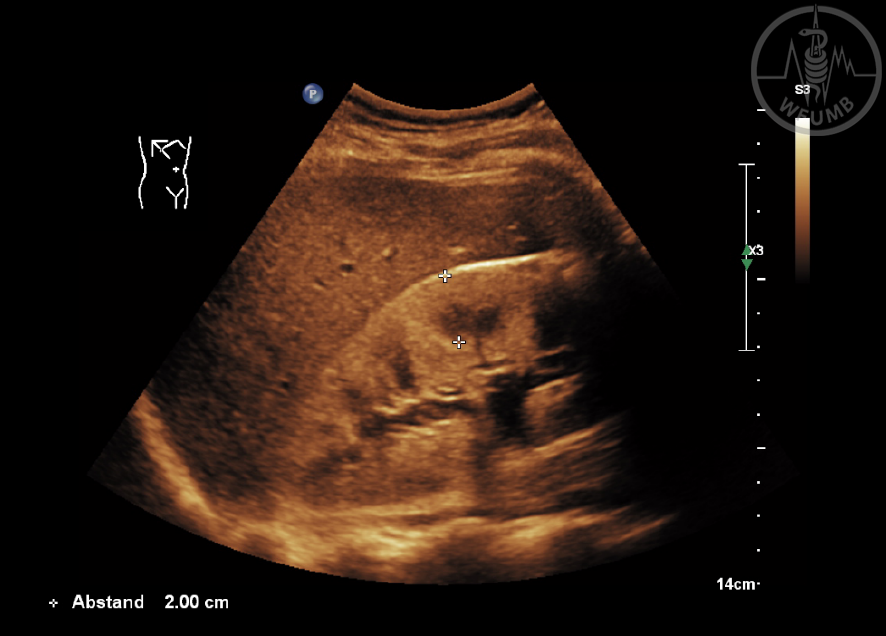
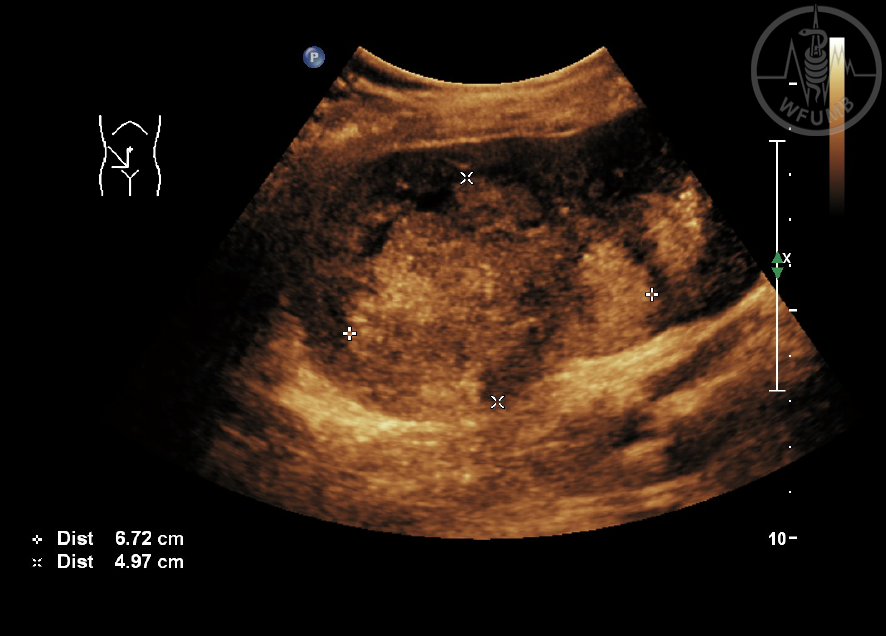
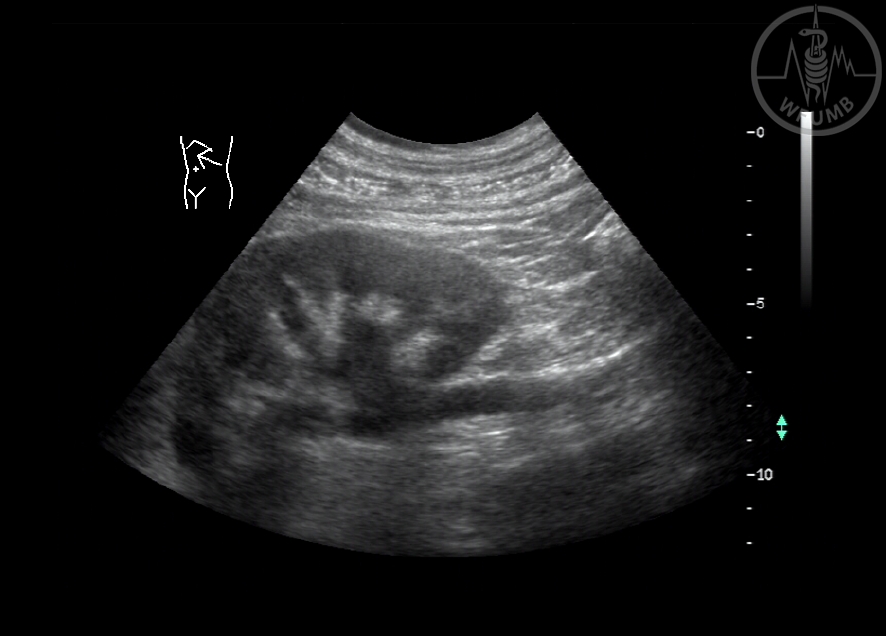
Fig 21.3
Examination of left (le) kidney in important prone position to visualise an echorich tumor dorsal of the kidney
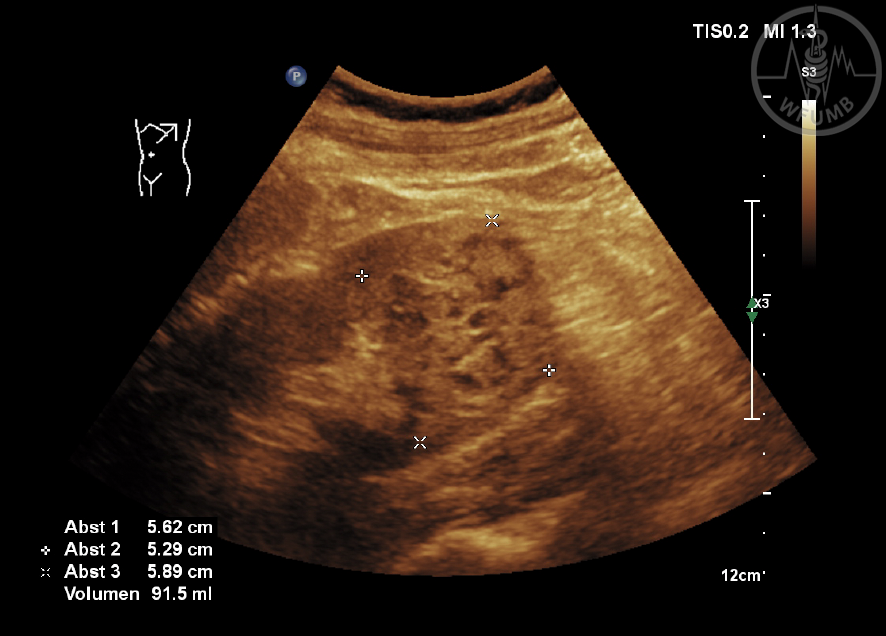
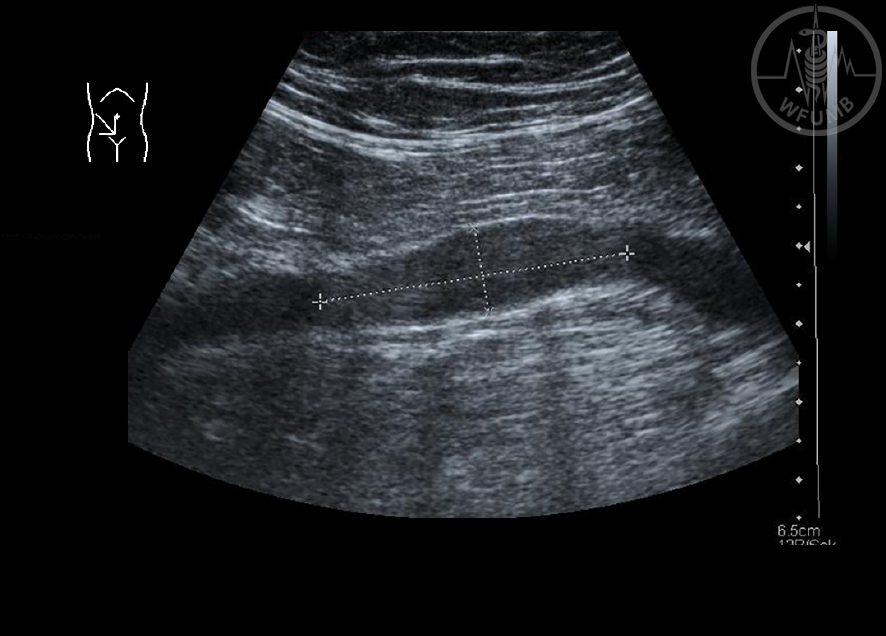
Fig 21.4a
Measurement of right kidney longitudinal
Fig 21.4b
Measurement of right kidney transversal and sagittal
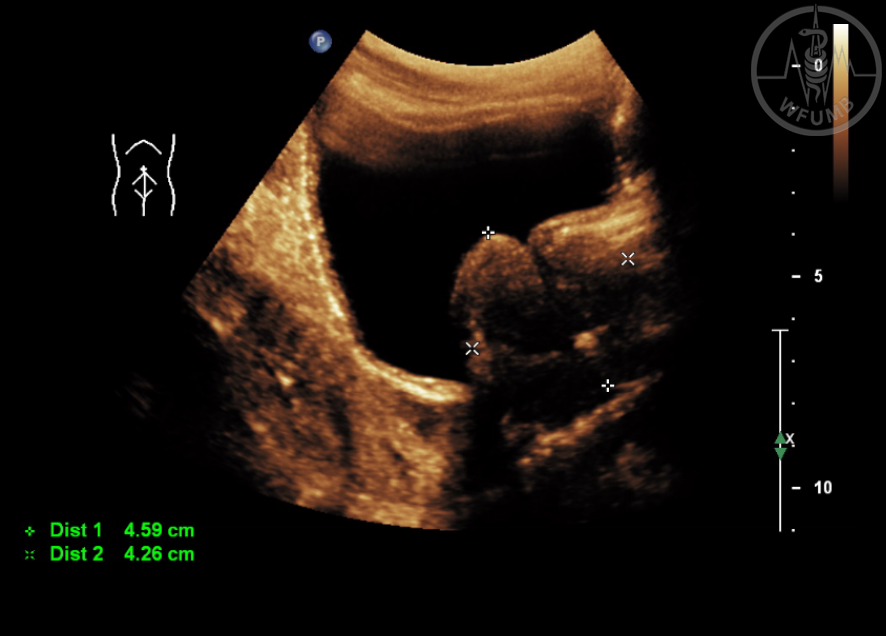
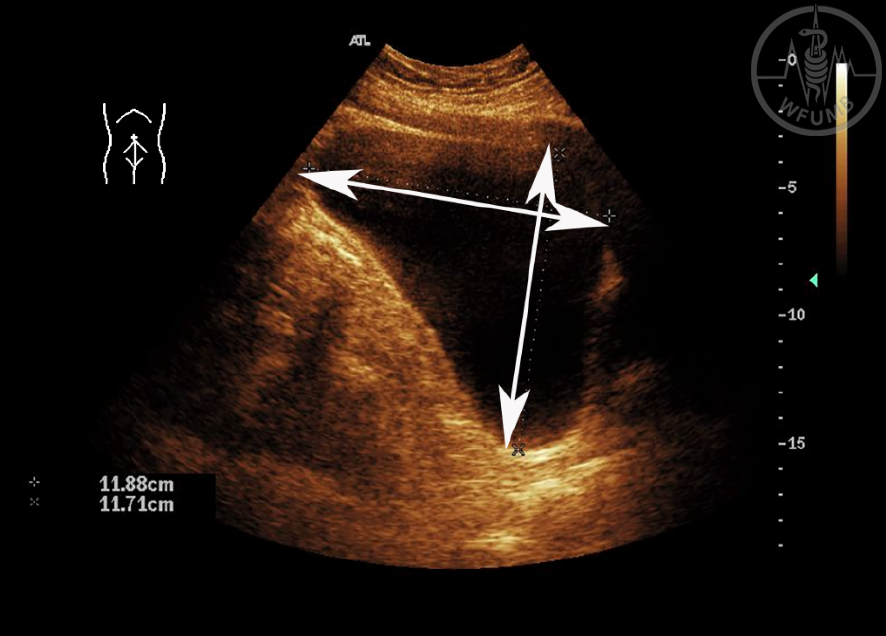
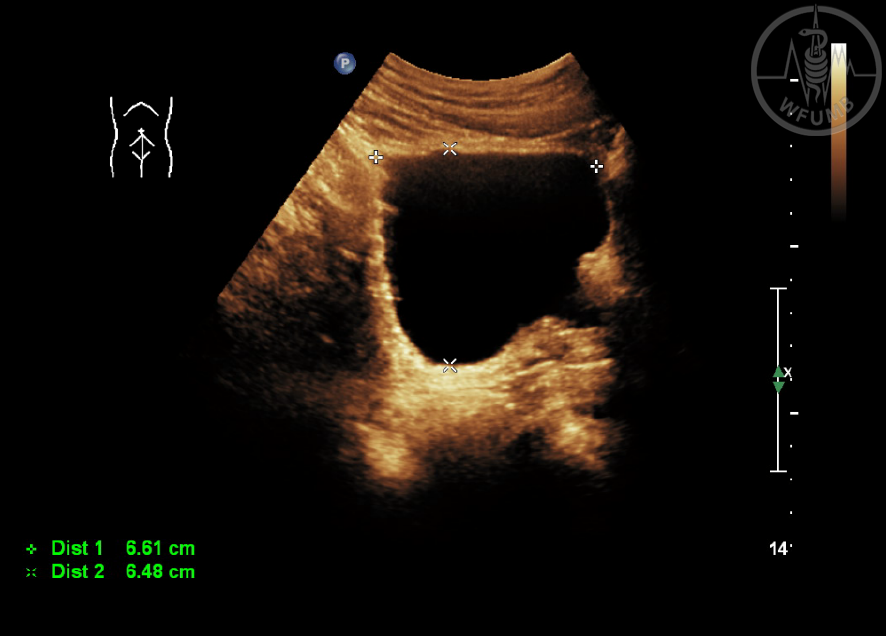
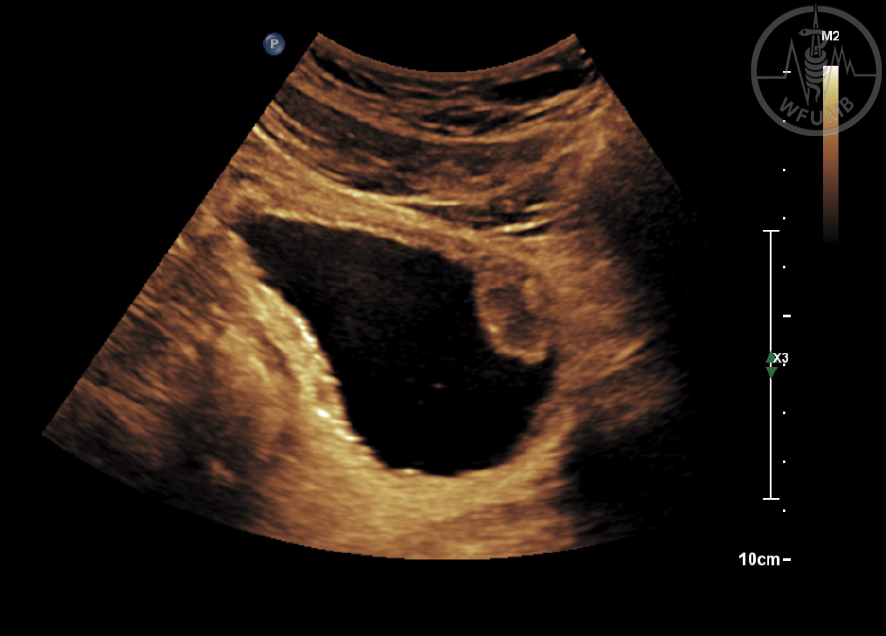
Fig 21.5a
Measurement of bladder and urine in longitudinal
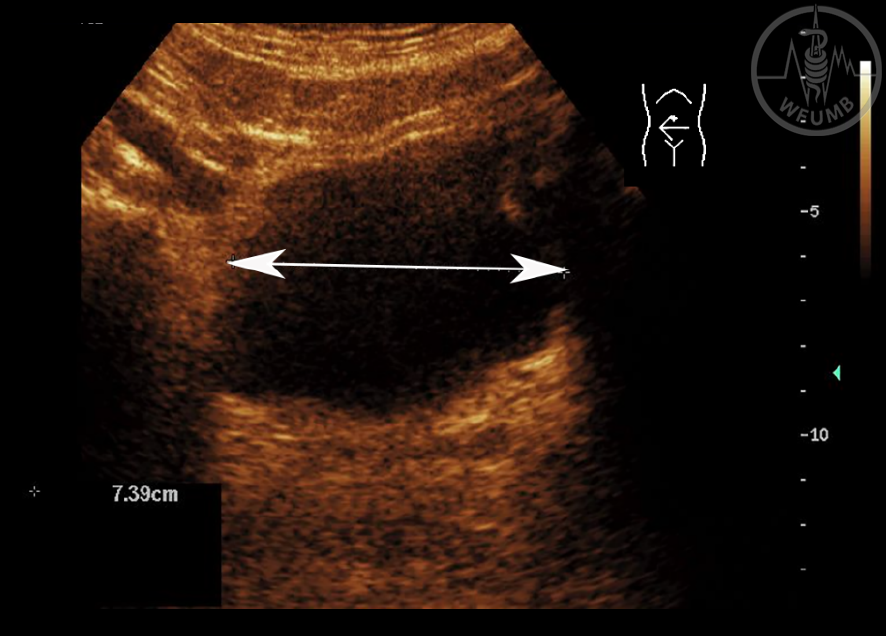
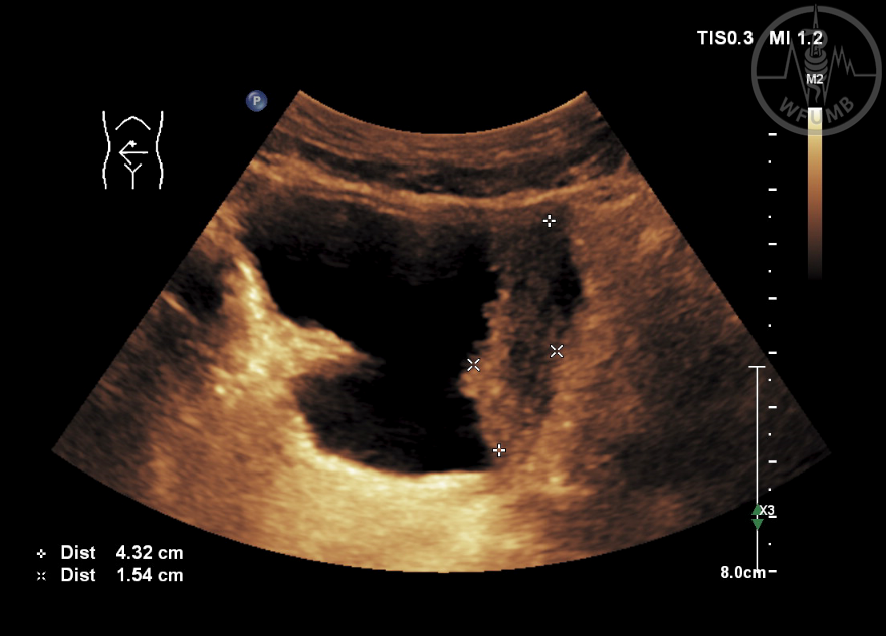
Fig 21.5b
Measurement of bladder and urine in transversal axis, used to measure residual urine
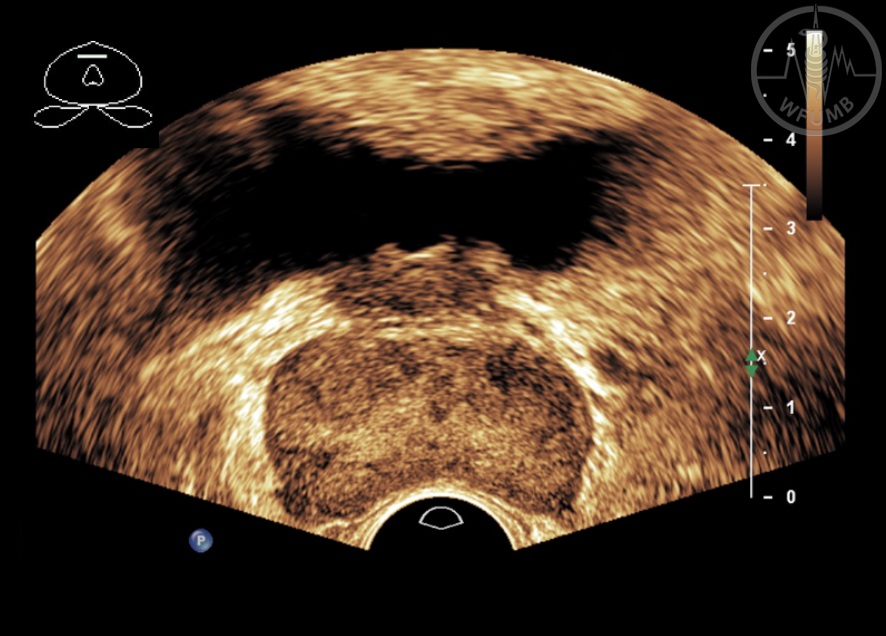
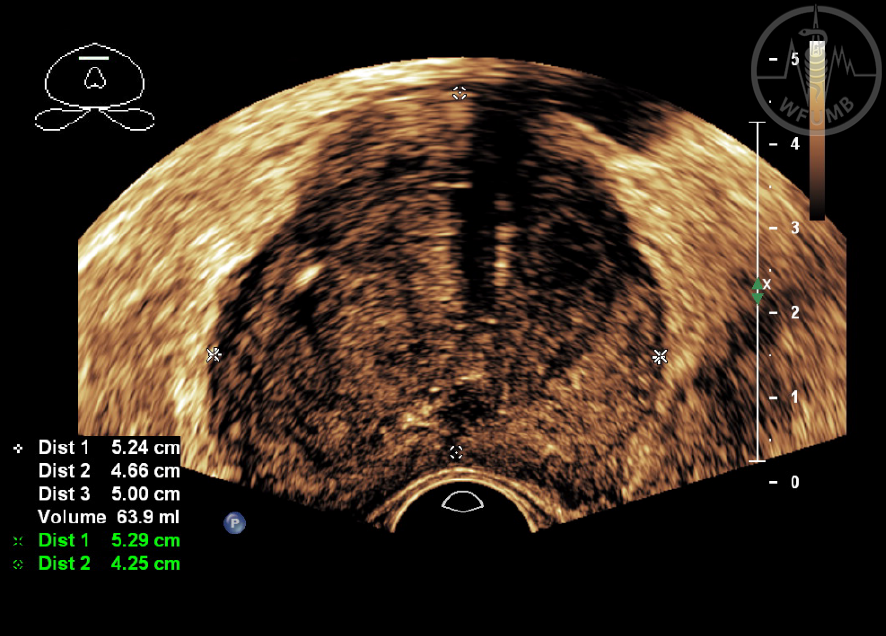
Fig 21.6a
Transvesical measurement of the prostate
Fig 21.6b
Transvesical assessment of the prostate after TUR (part of the prostate missing)
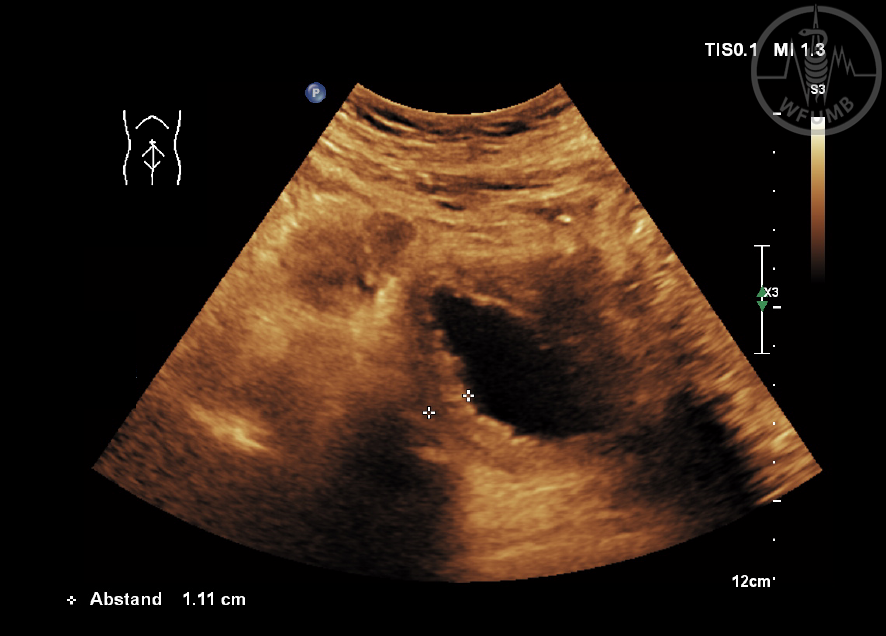
Fig 21.7a
Urinary obstruction grade 2 in renal colic caused by ureter stone
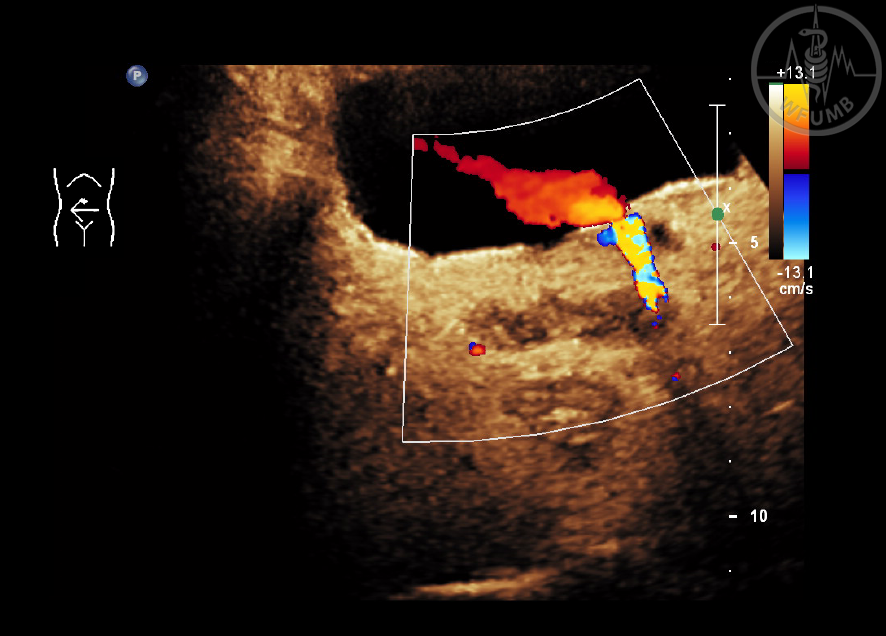
Fig 21.7b
Twinkling artefact in distal ureter before bladder, but positive urine jet on the right
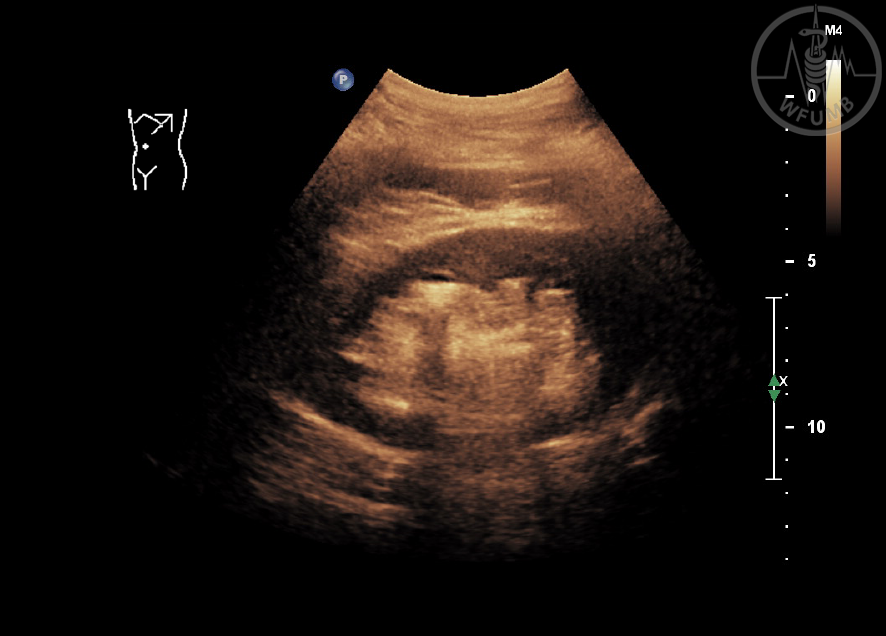
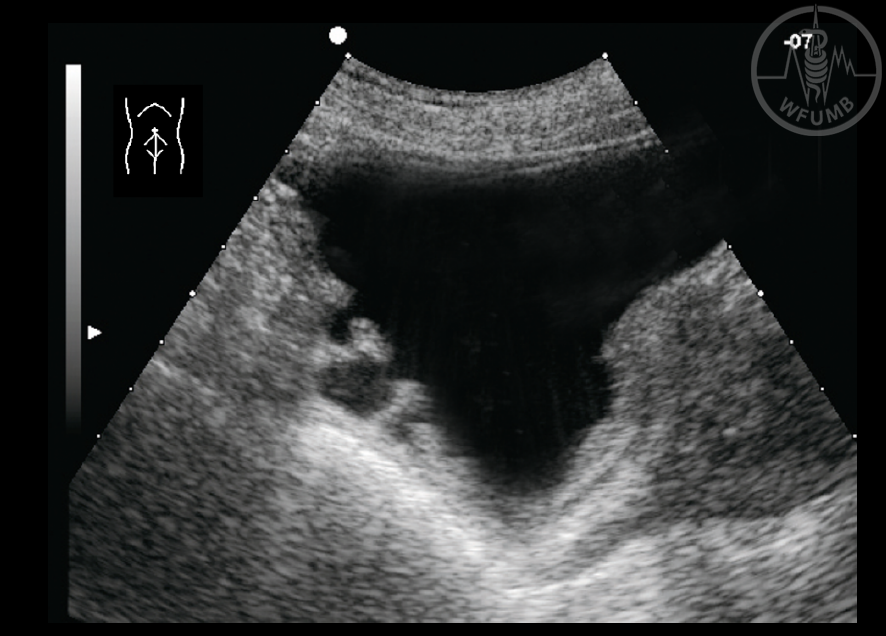
Fig 21.8a
Kidney with megacalices, a rare renal anomaly
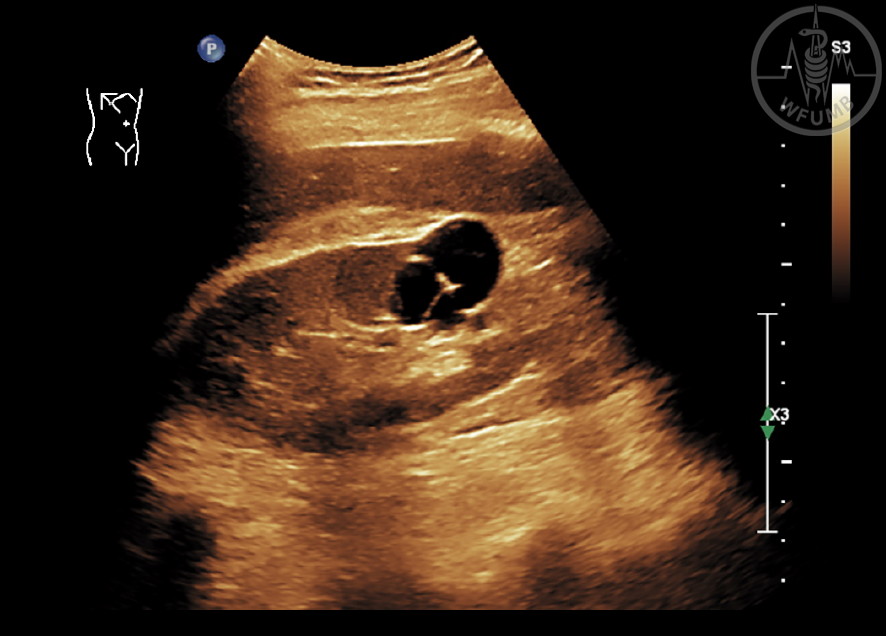
Fig 21.8b
A blind ending channel is found on the caudal ventral side of the bladder as a remnant of Urachus
Fig 21.9a
Acute glomerulonephritis with hepatorenal quotient is 0.76 and the quotient between the cortex and medulla is 2.37, which is significantly increased - post-infectious glomerulonephritis
Fig 21.9b
Chronic glomerulonephritis, IgA nephropathy diagnosed by biopsy turned into terminal renal insufficiency
Fig 21.10a
Gout kidney. Gout also leads to changes, namely calcifications in both the medullary pyramids and in the cortex
Fig 21.10b
Primary oxalosis. Very impressive pictures of a primary oxalosis, practically totally calcified kidney
Fig 21.12b
Bosniak IV complex renal cyst. Arrow shows solid part in cyst
Fig 21.13a
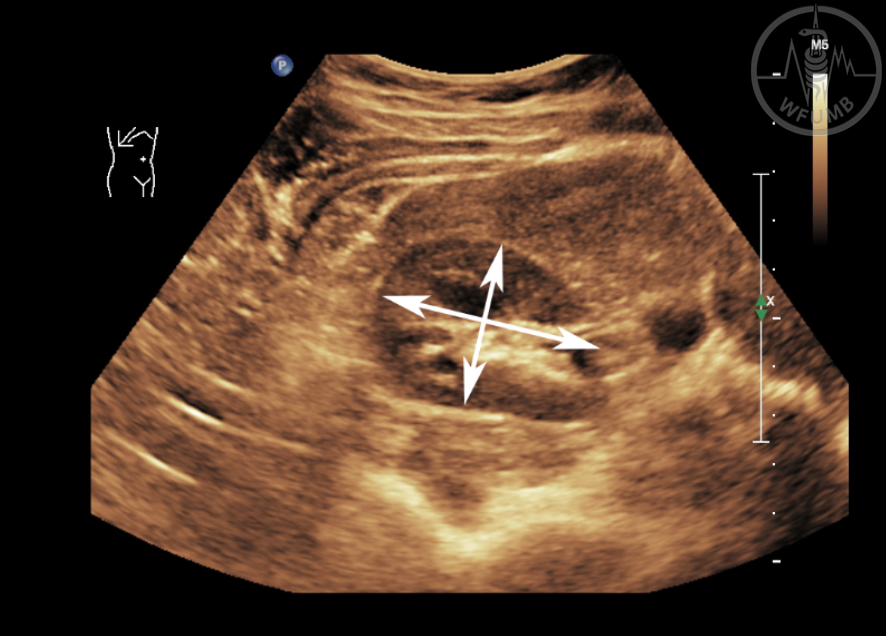
Problems are caused by the so-called renal parenchymal cones, which can look like a real tumor (inflammatory pseudotumor)
Fig 21.13b
Angiomyolipoma (AML) is usually a hyperechoic tumour made up of adipose tissue, blood vessels and smooth muscles
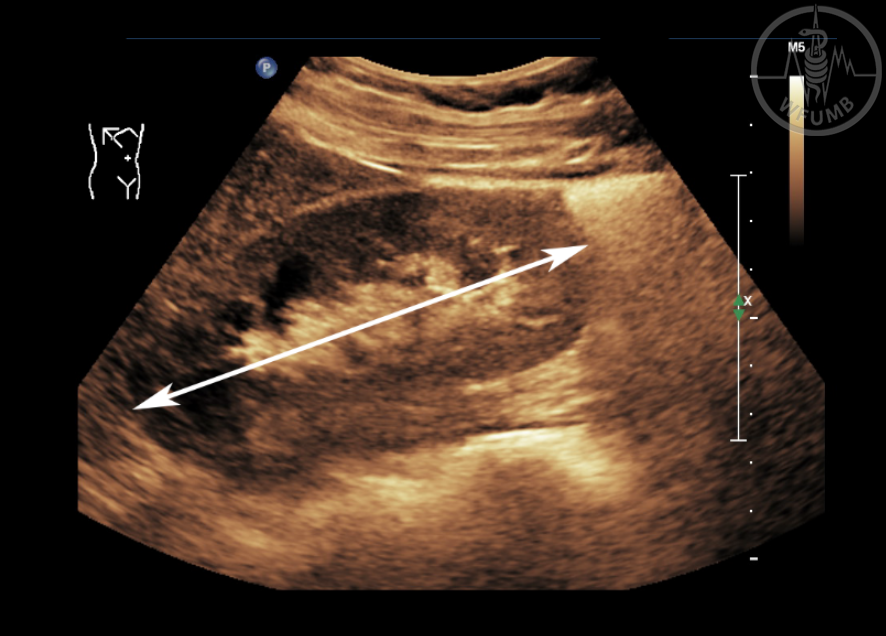
Fig 21.14
Malignant tumor of lower pole of the left kidney -
clear cell renal cell carcinoma (RCC)
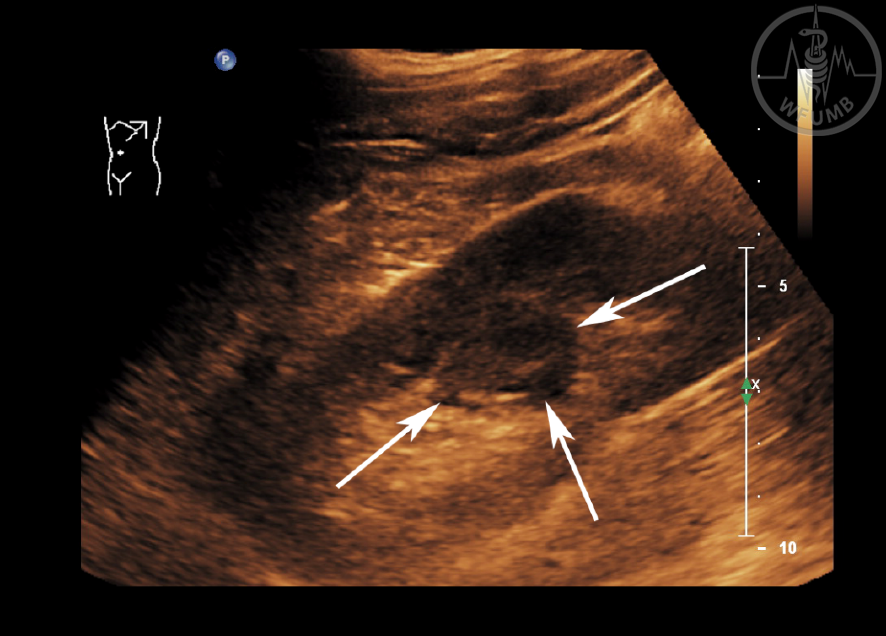
Fig 21.15
Clear cell renal cell carcinoma (RCC). In larger tumors, there are larger inhomogeneities in the B-scan. Pseudo cystic or necrotic areas are very clearly visible in CEUS (unenhancing areas)
Fig 21.16
Chromophobic renal cell carcinomas (CRCC) are difficult to distinguish from oncocytomas. They are homogeneous, isoechogenic and they also behave similarly at CEUS
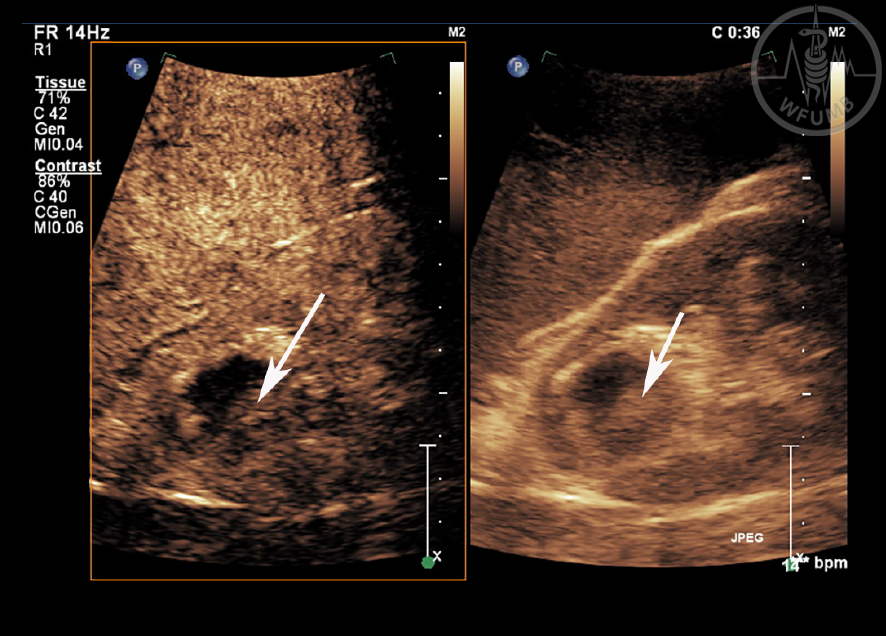
Fig 21.17
Papillary renal cell carcinomas (PRCC) are mostly homogeneous and hypoechoic; in CEUS (left panel, arrows) they are weakly perfused
Fig 21.18
Hemangiosarcoma is a very rare tumor, here observed in a kidney transplant
Fig 21.19
Hematoma - A fresh hematoma can be hyperechoic, later hypoechoic
Fig 21.20a
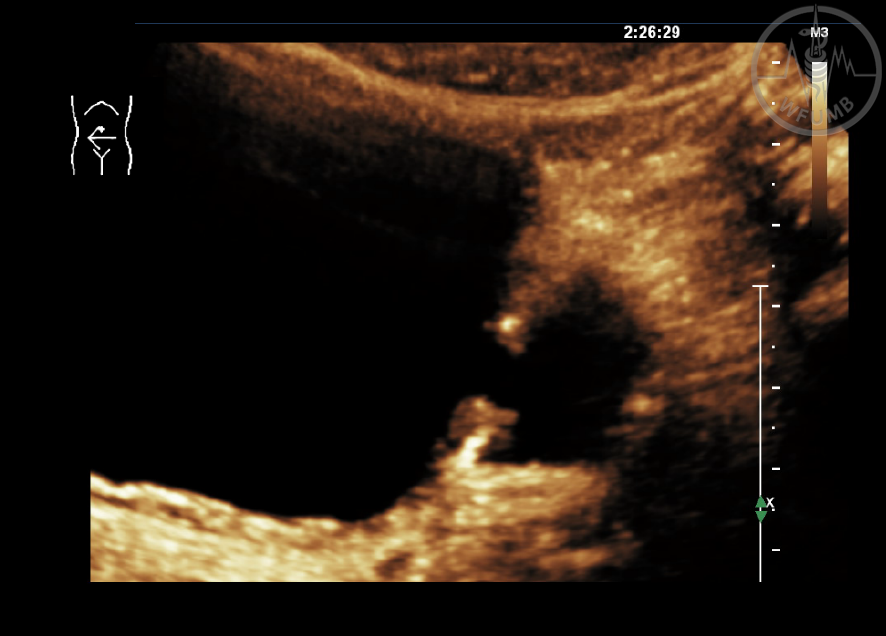
Urinary obstruction Grade 2 dilatation is seen as a dilated ureter and a fornix angle of at least 90 degrees
Fig 21.20b
Final stage, i.e. congestion grade IV (hydronephrosis) with practically no kidney cortex
Fig 21.21
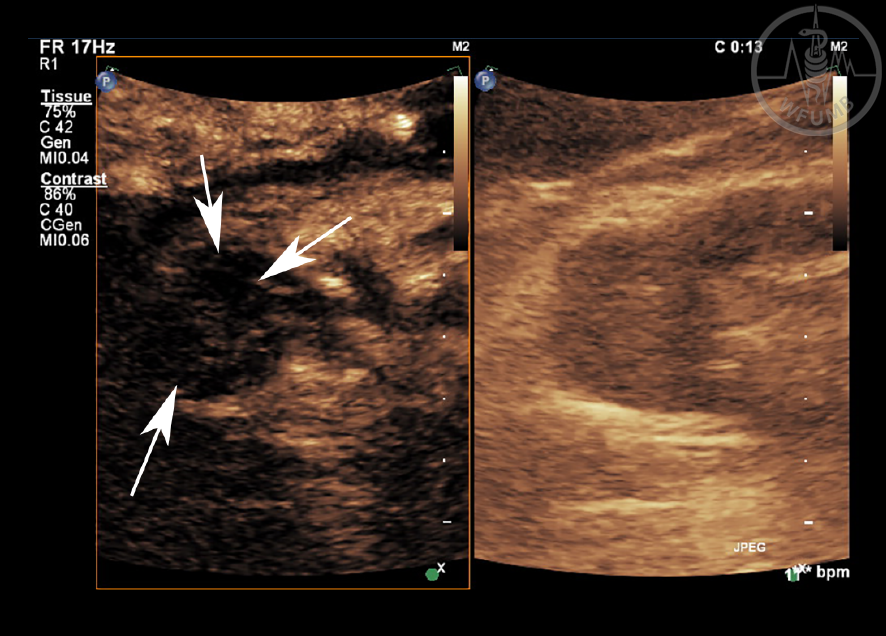
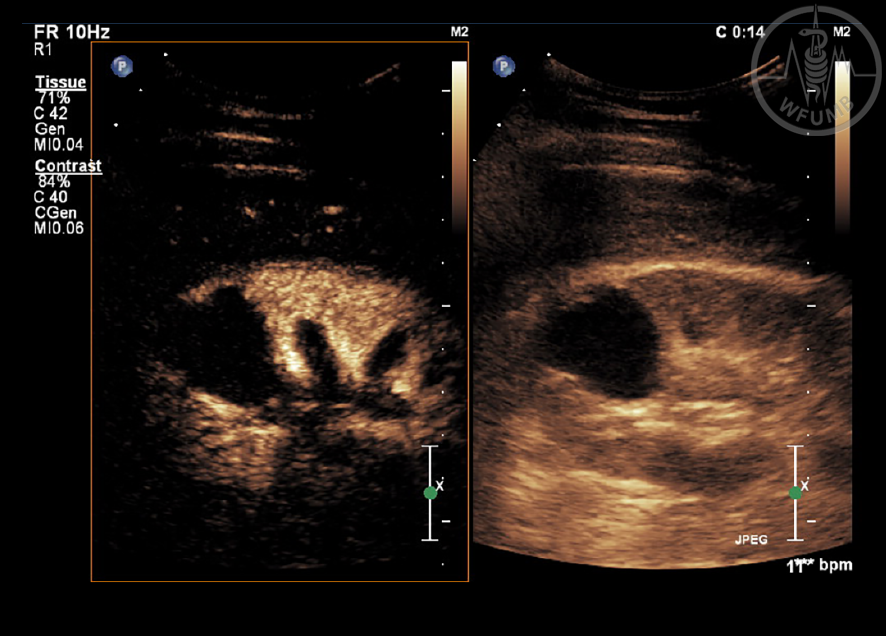
Calyx diverticulum, better visualized with
CEUS (left panel)
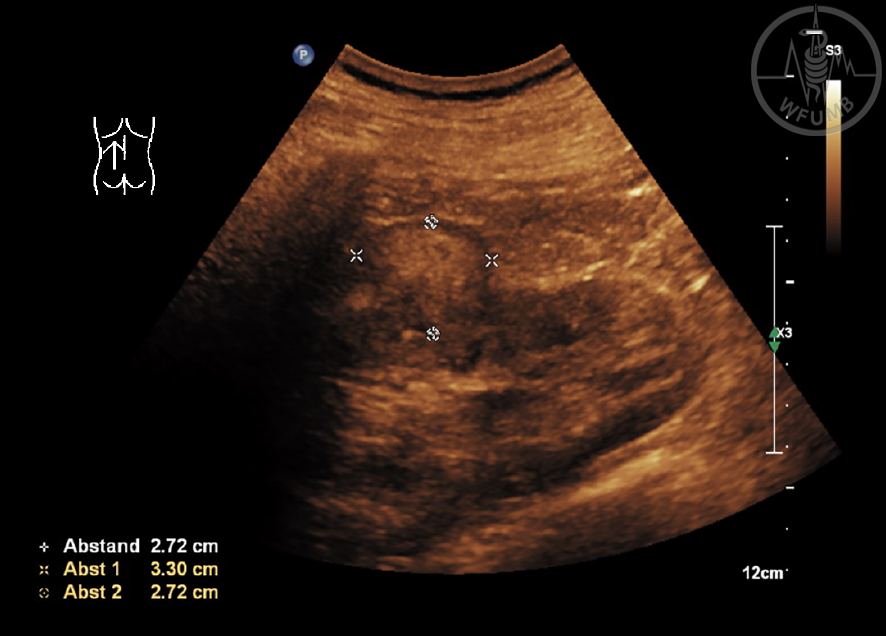
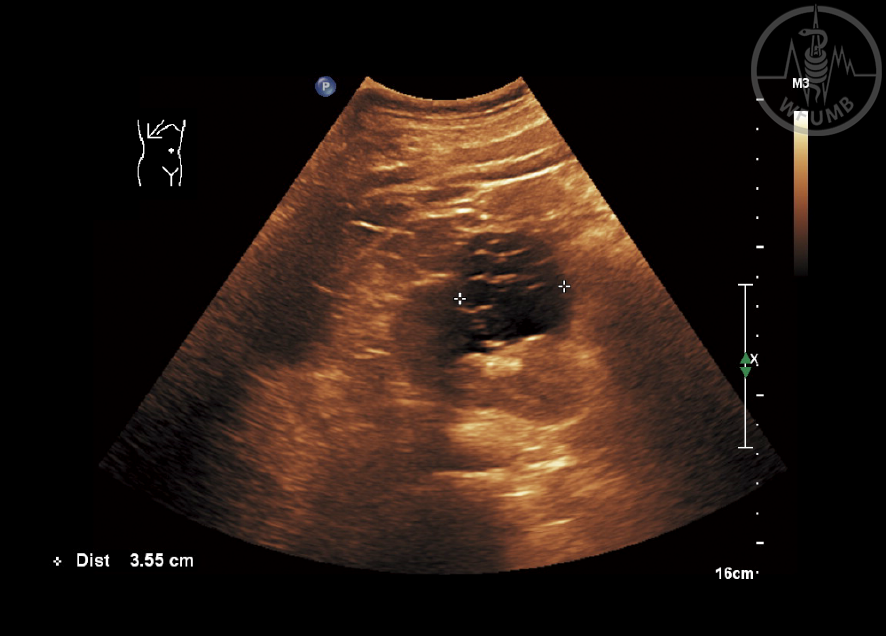
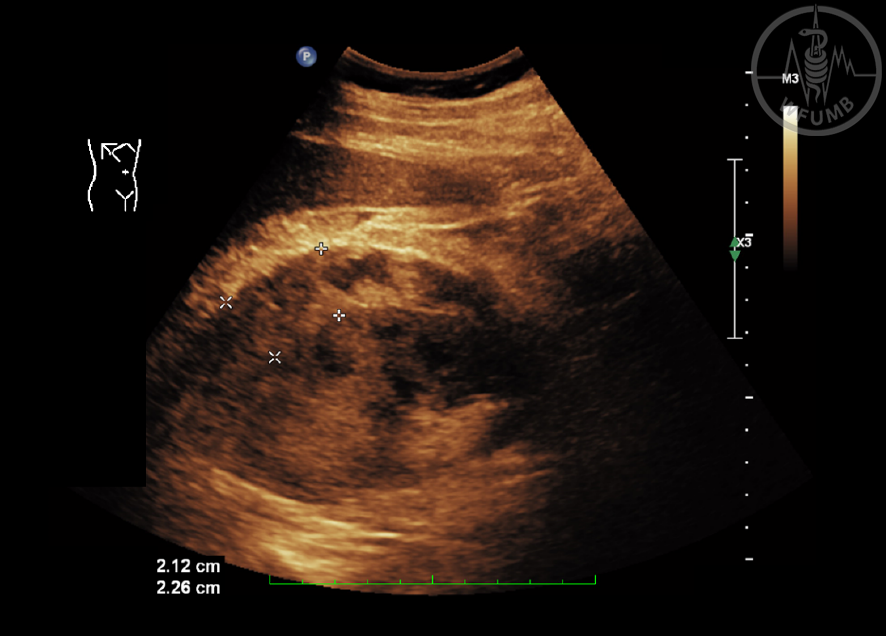
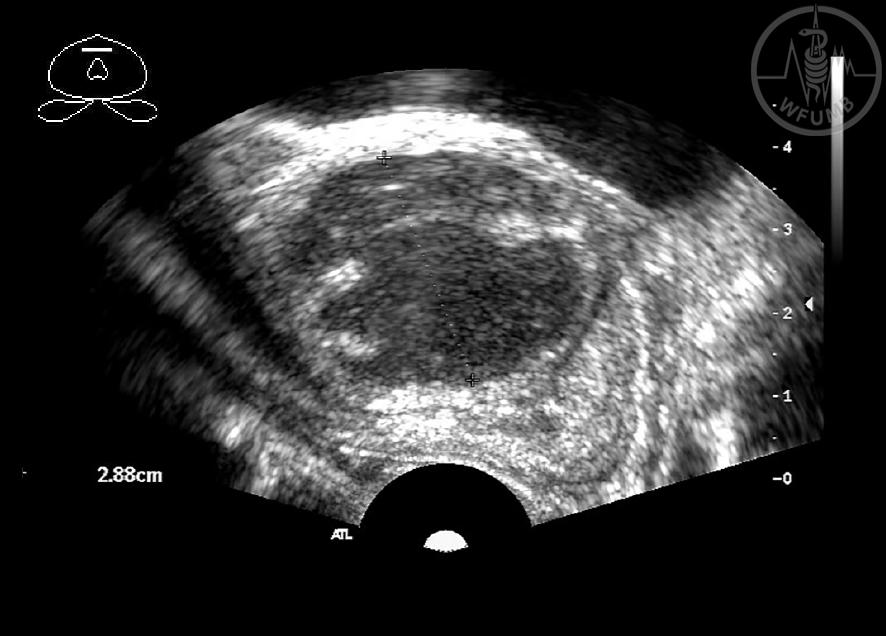
Fig 21.22
Kidney pelvis tumor (marker) can appear relatively hidden in an enlarged calyceal system
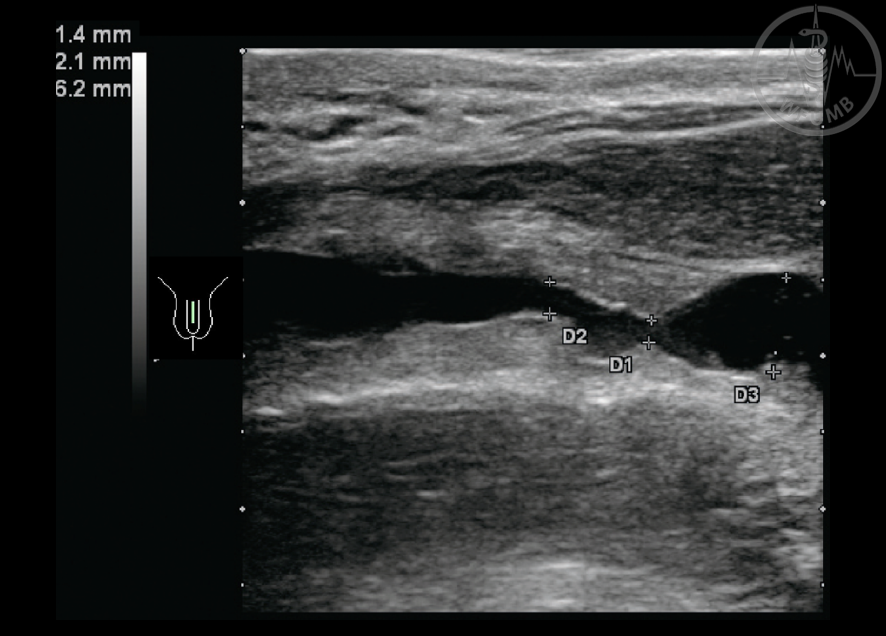
Fig 21.23a
Hydroureter or dilated ureter caused by ureteric stones
Fig 21.23b
Example of ureter tumor, seldom diagnosed by US
Fig 21.24a
Bladder diverticula can be congenital or acquired
Fig 21.24b
Inflammatory pseudotumor sometimes looks like a tumor
Fig 21.25a
Interstitial cystitis is a special form of cystitis with characteristic bladder wall thickening
Fig 21.25b
Trabecula bladder in obstructive uropathy, especially in prostatic hyperplasia
Fig 21.26a
Bladder tumor – solid mass in the bladder lumen. Most of them are malignant
Fig 21.26b
Bladder tumor – solid mass in the bladder lumen (longitudinal axis)
Fig 21.27a
Stricture of urethra
Fig 21.27b
Calcification/stone in the urethra (using high-frequency probe!)
Fig 21.28a
Harmless thin-walled prostate cysts pose no problems for the patient
Fig 21.28b
In transrectal examination hypoechoic, semi-liquide formation corresponding to a prostate abscess
Fig 21.29a
Prostate calcifications often found after prostatitis
Fig 21.29b
In BPH, dystrophic calcifications on the border between transitional zone and peripheral zone (twinkling artefact) are often found
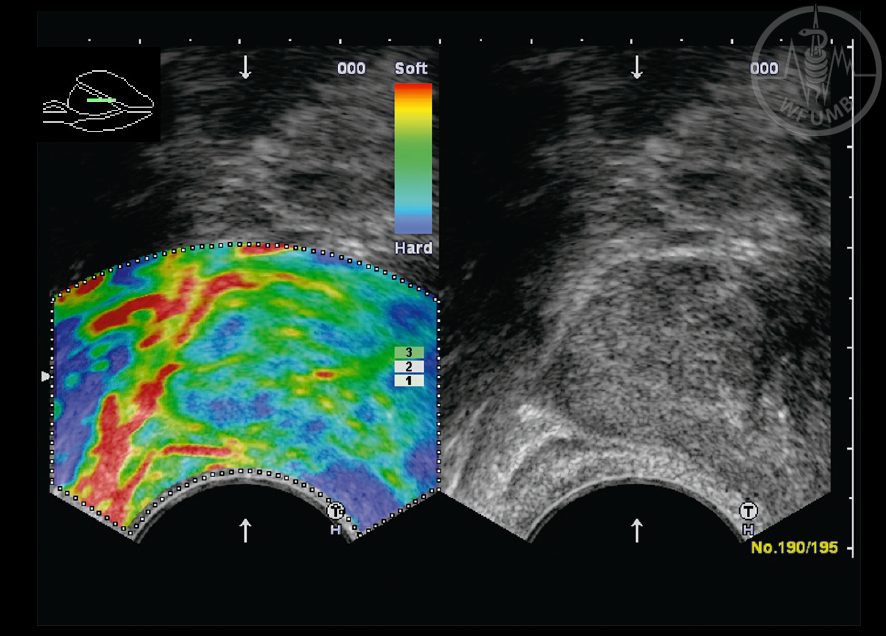
Fig 21.30
Elastography in prostate carcinoma. Carcinomas are harder (blue), than the surrounding area
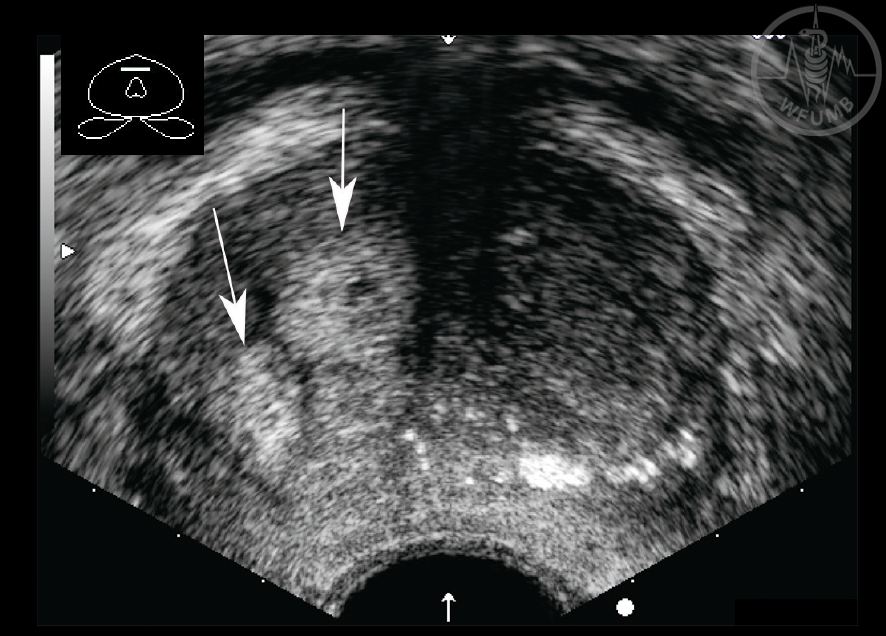
Fig 21.31
Two hyperechogenic nodules correspond to benign prostate adenomas (arrows)
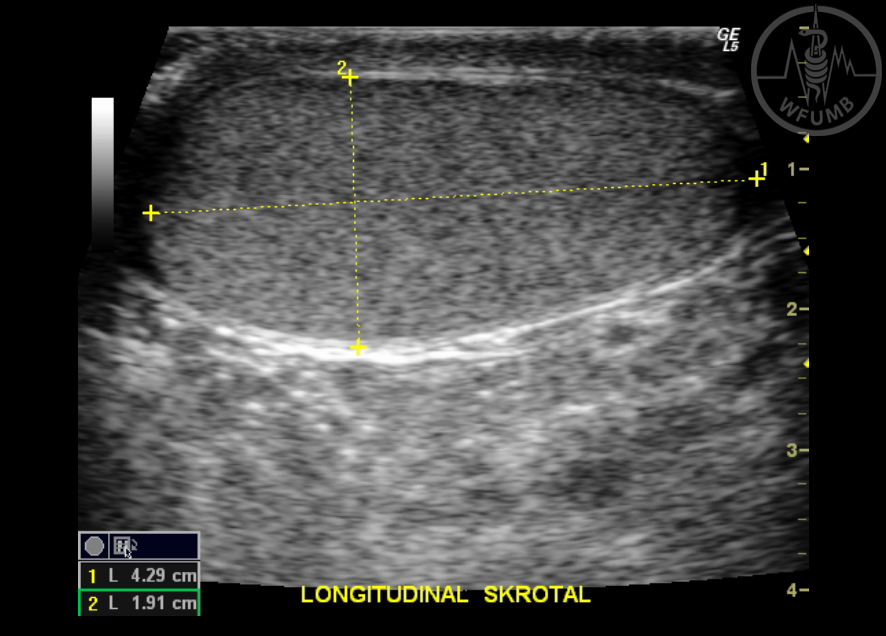
Fig 21.32a
Normal testicular sono-anatomy on longitudinal view, shows normal homogenous echogenicity throughout, with exception of peripherally located hyperechoic mediastinum
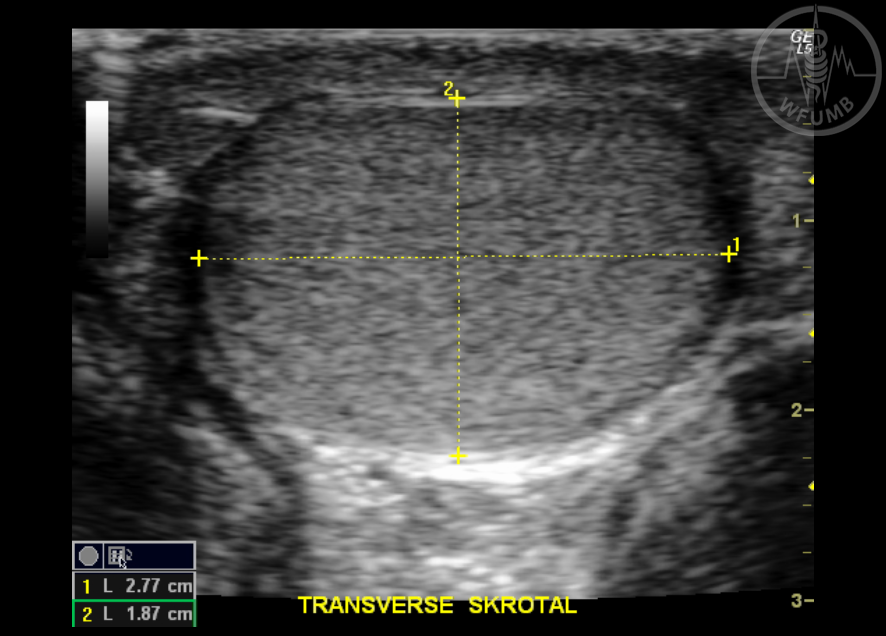
Fig 21.32b
Normal testicular
sono-anatomy on transverse view
Fig 21.33a
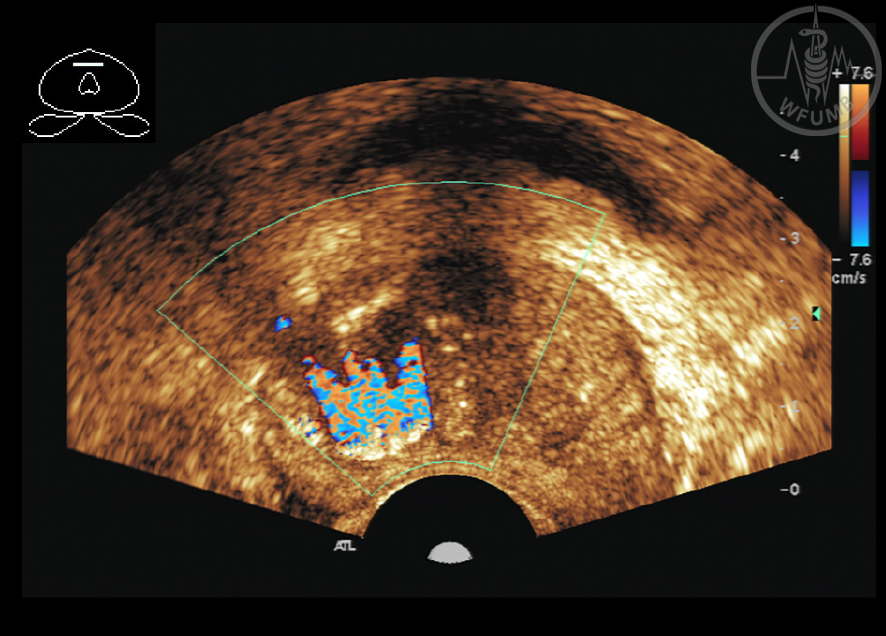
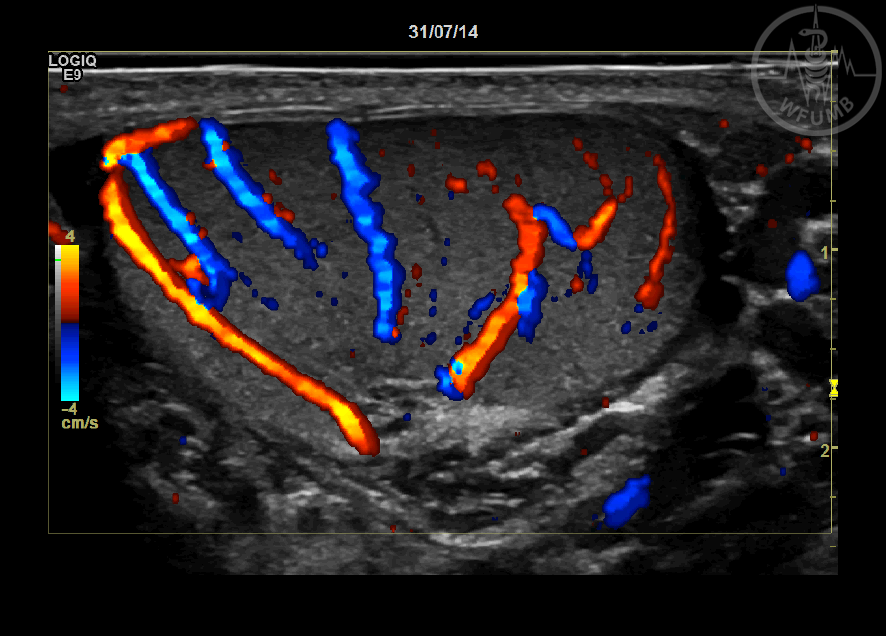
CD show branches of centripetal arteries which supply blood to the testicular parenchyma and the capsular arteries which located on the peripherally and enter the testis and travel toward the mediastinum
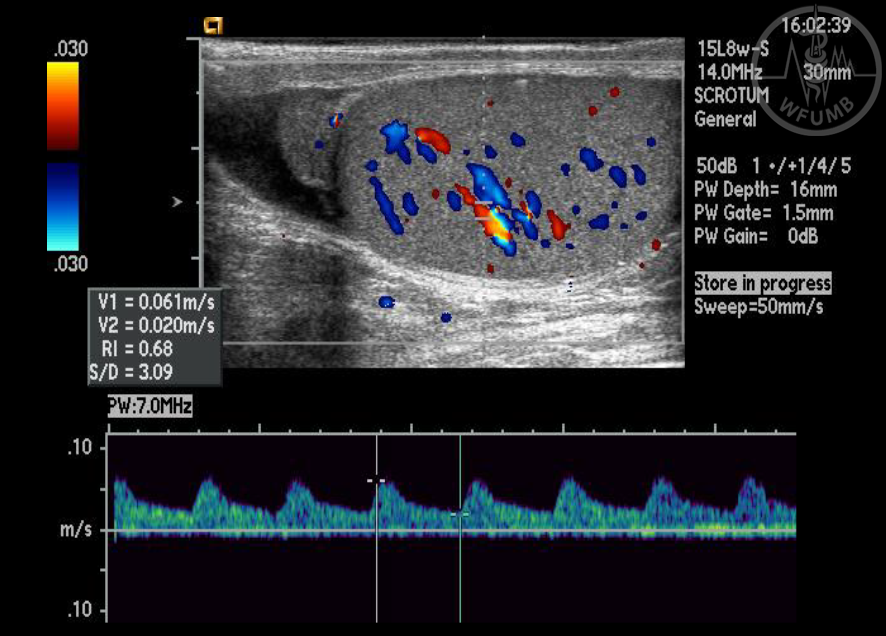
Fig 21.33b
CD and PWD (Pulse Wave Doppler) of normal testis
Fig. 21.34a
Tunica albuginea cyst. Longitudianl view of the testis show typically peripherally located simple cyst
Fig 21.34b
Moderate size simple testicular cyst. Longitudinal view show an anechoic structure with strong posterior acoustic enhancement in the testicular parenchyma
Fig 21.35a
Testicular Infarction. Longitudinal view of the testis show multiple focal hypoechoic areas
Fig 21.35b
Testicular Microlithiasis. Longitudinal view of the testis demonstrats scattered small bright hyperechoic points without acoustic shadowing. Two small complex cyst are also identified
Fig 21.36a
CD of the left torsed testis shows no detectable blood flow on the testicular parenchyma
Fig 21.36b
Longitudinal view of left torsed testis in a different patient. CD shows no detectable blood flow in the torsed testis and also shows increased flow in the wall of the scrotum
Fig 21.37a
Seminoma. The testis is swollen and a lobulated, hypoechoic nodule was seen associated with microliths. Reactive hydrocele also noted
Fig 21.37b
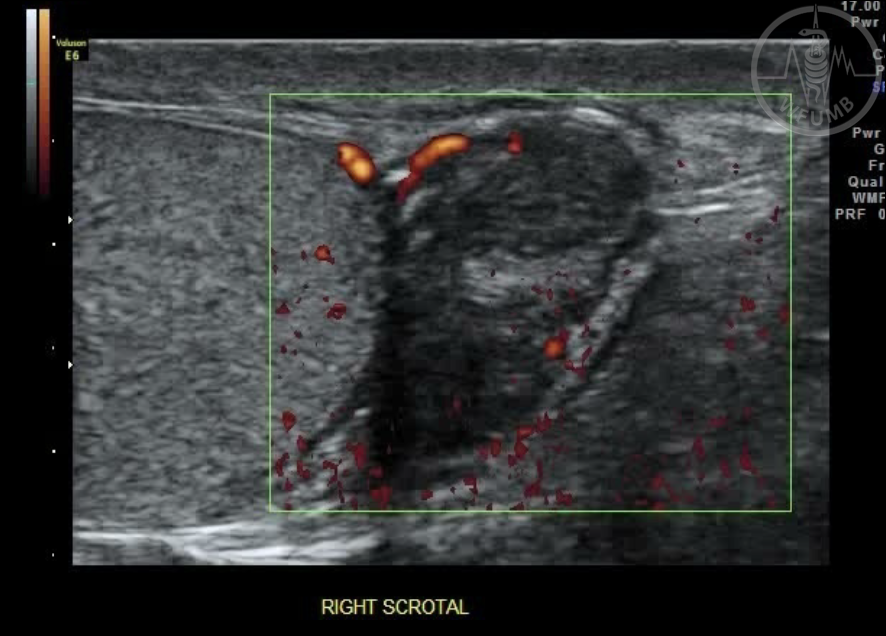
Small solid testicular lesion, Longitudinal view of the testis shows an oval hypoechoic lesion with mildly irregular border.
CD shows blood flow in the periphery of the lesion
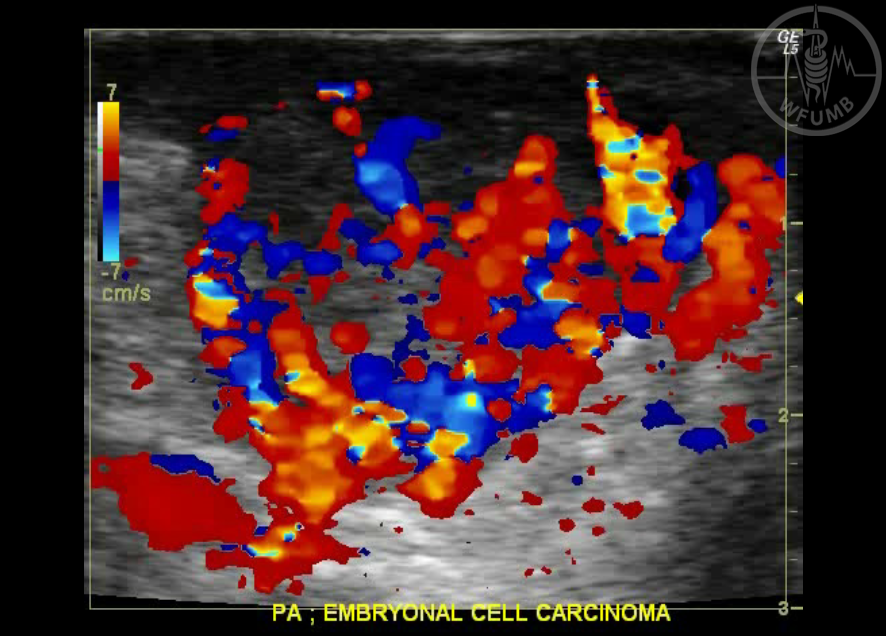
Fig 21.38a
Embryonal cell carcinoma. Longitudinal view of the testis shows an oval hypoechoic lesion with a disorganized hypervascular pattern on CD, also noted that central necrosis is present
Fig 21.38b
Embryonal cell carcinoma. Longitudinal view of the testis shows an oval hypoechoic lesion with a disorganized hypervascular pattern on CD, also noted that central necrosis is present
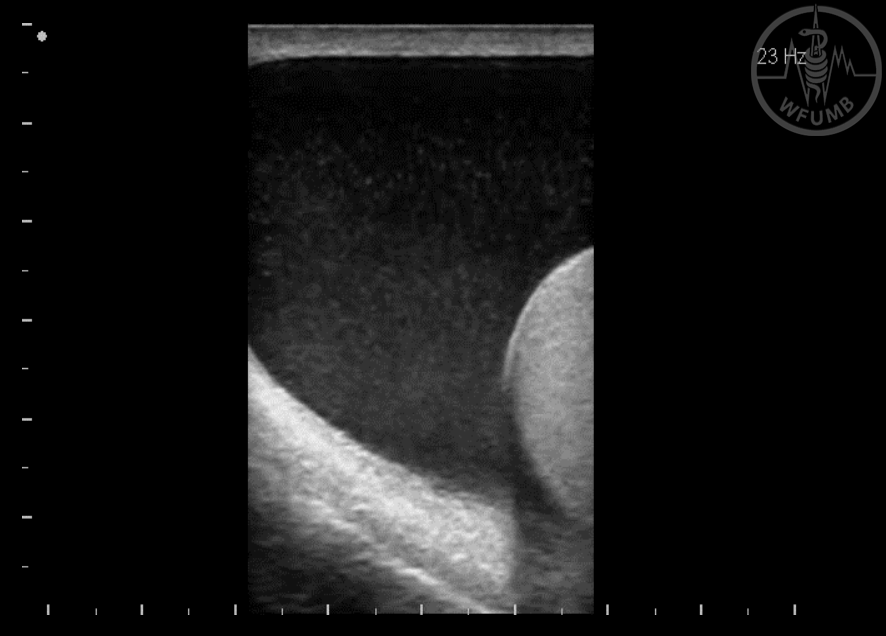
Fig 21.39a
Large hydrocele with diffuse low-level echoes
Fig 21.39b
Spermatocele. Longitudinal view shows a moderate size spermatocele. on the right epididymal head, however a epididymal cyst may also form in the epididymal head, with similar US features
Fig 21.40a
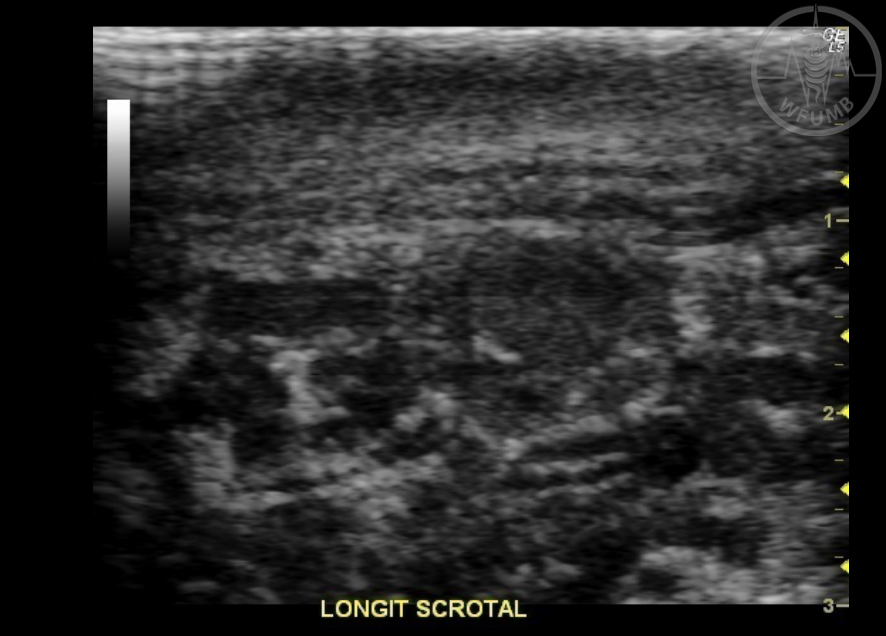
Adenomatoid tumor of the epididymal tail. Most of this benign tumor will appear as a solid hypoechoic inhomogenous lesion
Fig 21.40b
Minimal detectable blood flow may be seen on Color Flow Imaging
Fig 21.41a
Varicocele. Longitudinal view at rest shows tortuous tubular structures located on the posterior aspect of the testis
Fig 21.41b
During the Valsalva maneuver, minimally dilated veins posterior to the testis with augmented venous flow are seen
Fig 21.42a
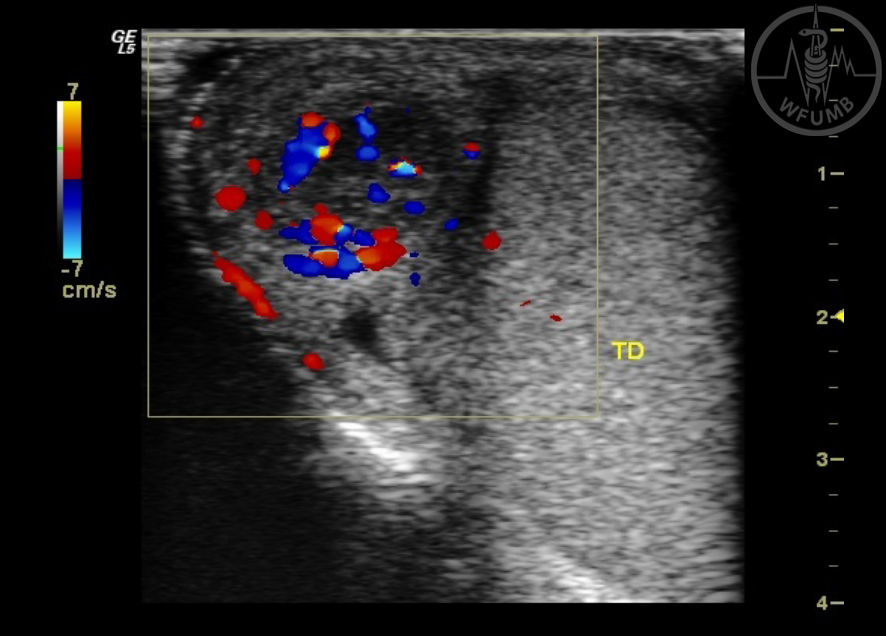
Acute epididymitis. A swollen epididymal head was noted
Fig 21.42b
Hypervascularisation of the epididymis head is seen in CD
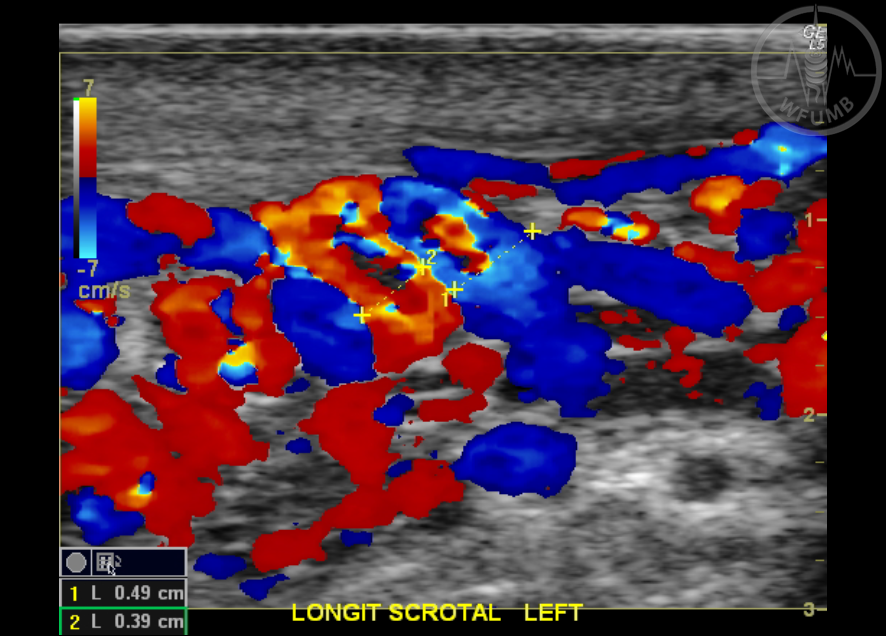
Fig 21.43a
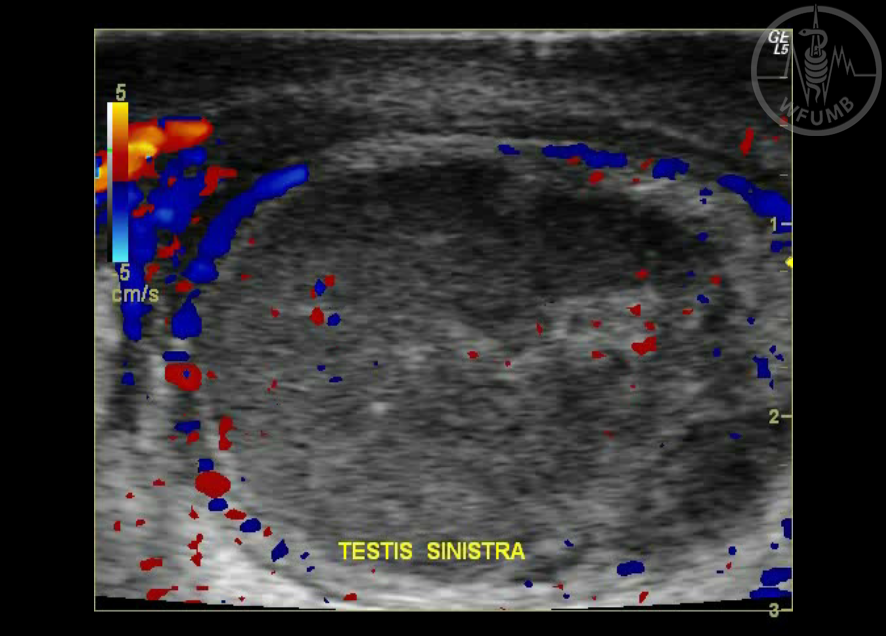
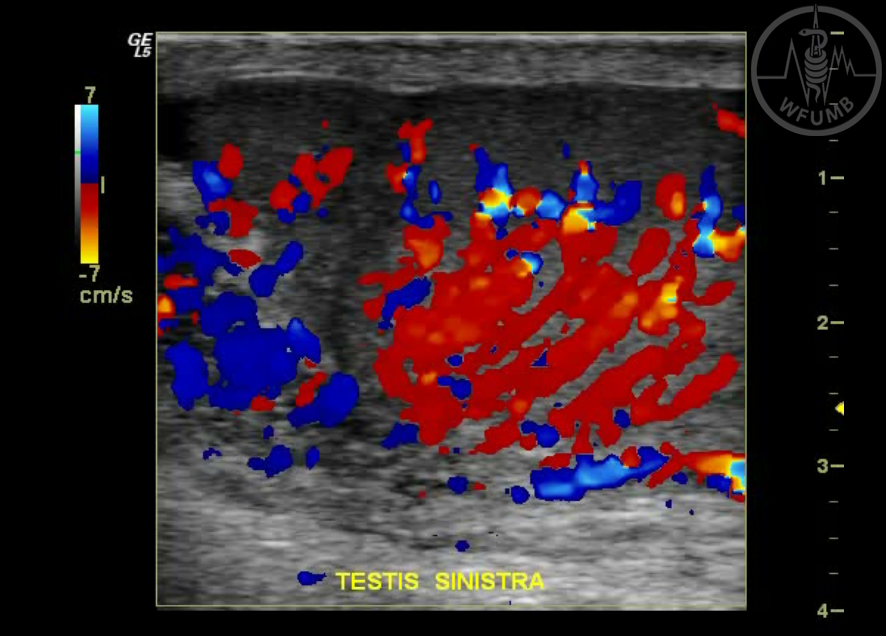
Left acute epididymo- orchitis. This patient has an acute left scrotal pain, longitudinal view of the left testis shows enlargement and swollen left testis with marked hyperaemia and asymmetry in perfusion
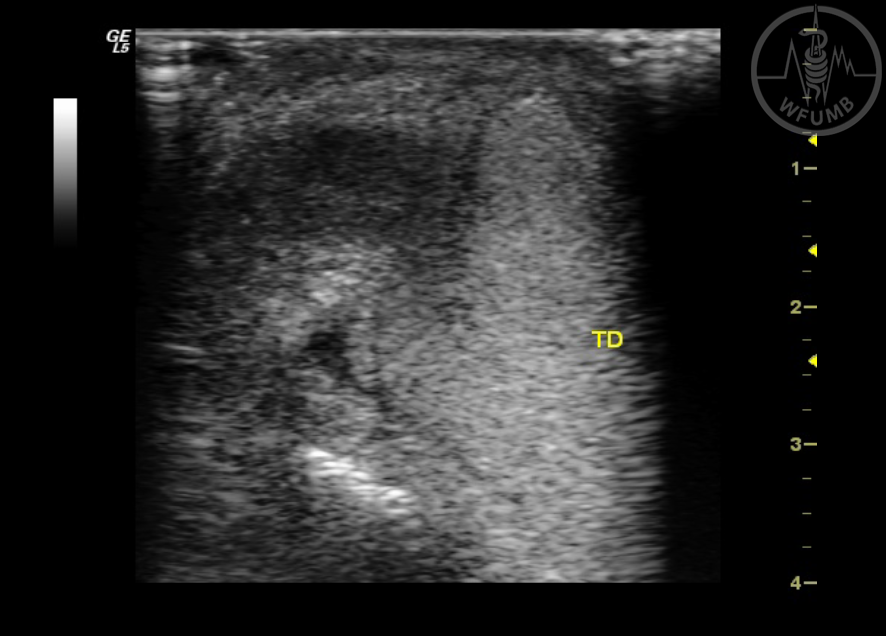
Fig 21.43b
CD of the normal right testis of the same patient