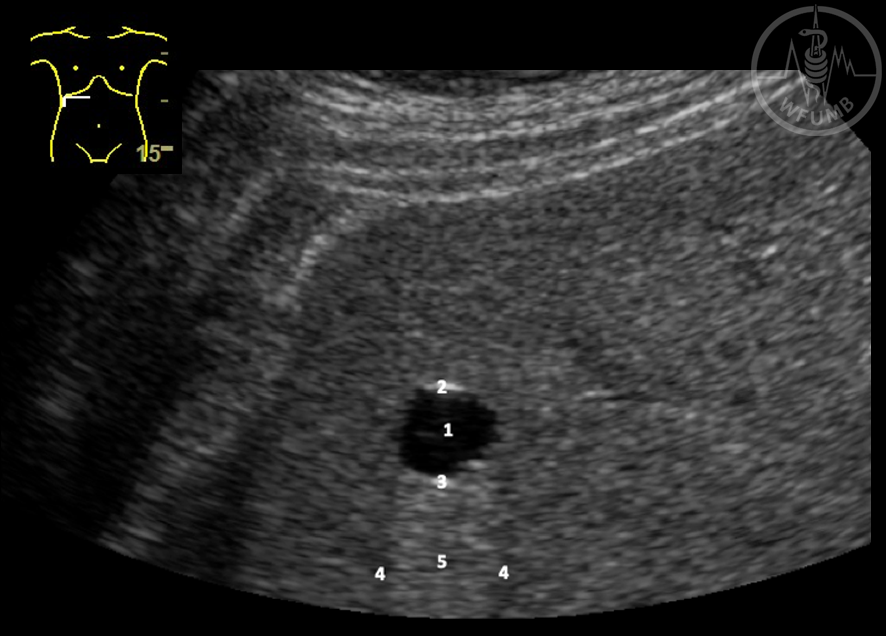
Fig 13.2.1 Liver cyst
Liver cysts are characteristically round, anechoic (1), smoothly delineated FLL with hyperechoic anterior (2) and posterior (3) wall, refraction shadows at their edges (4), a strong posterior wall echo (4) and post-cystic enhancement (5) resulting from an intensity difference between the beam intensity deep to the cysts and in the cysts. Transverse view of the pancreas - normal echogenicity. The left liver lobe was used as the acoustic window.
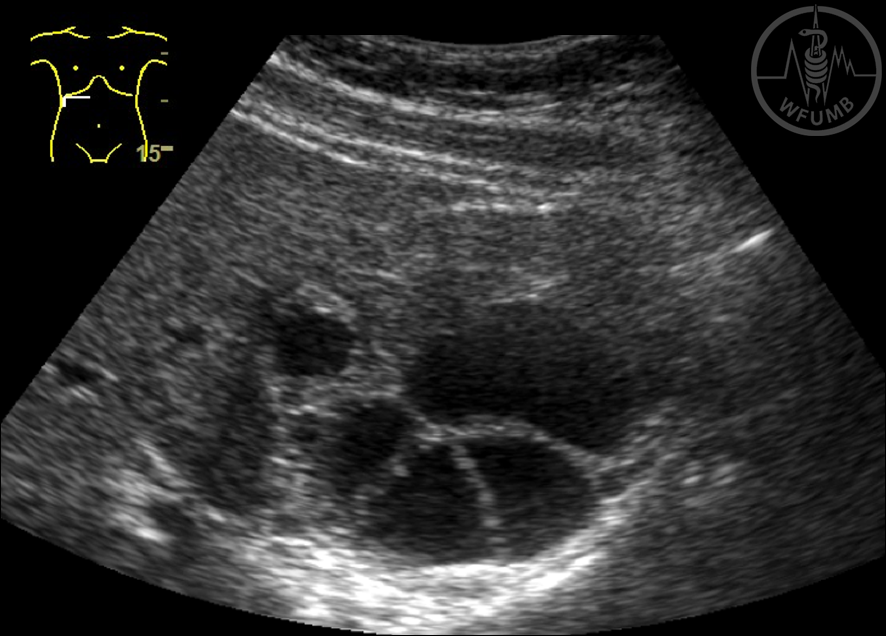
Fig 13.2.2 Hydatid cyst
Hydatid cyst, stage 3, cyst in the cyst pattern.
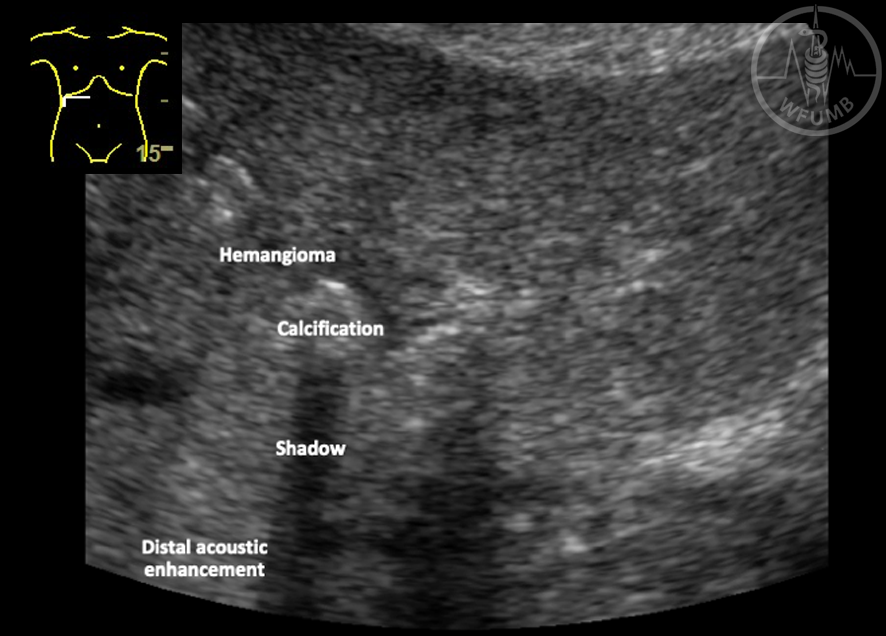
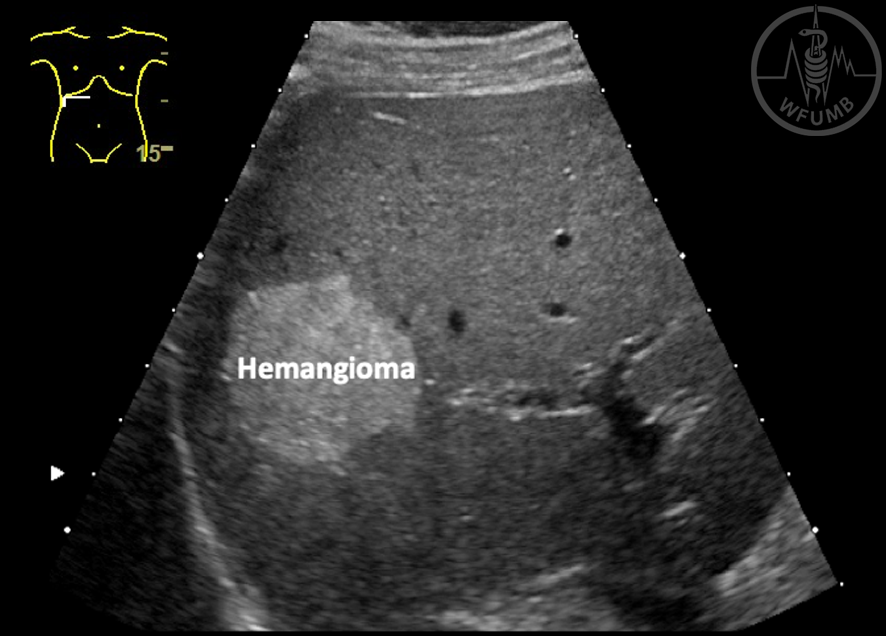
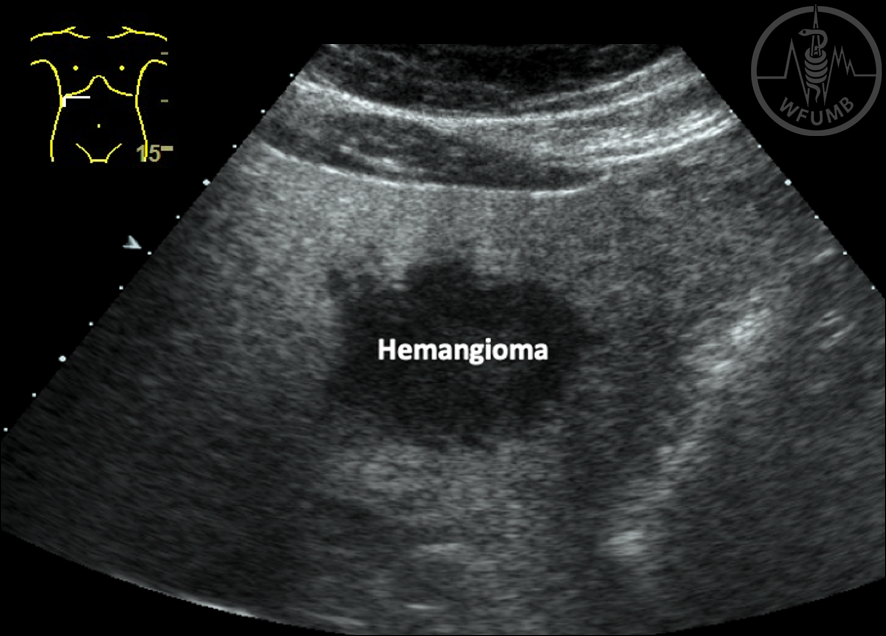
Fig 13.2.3 Calcification
Calcification is shown with shadowing. Next to the calcification an isoechoic hemangioma is shown with posterior acoustic enhancement
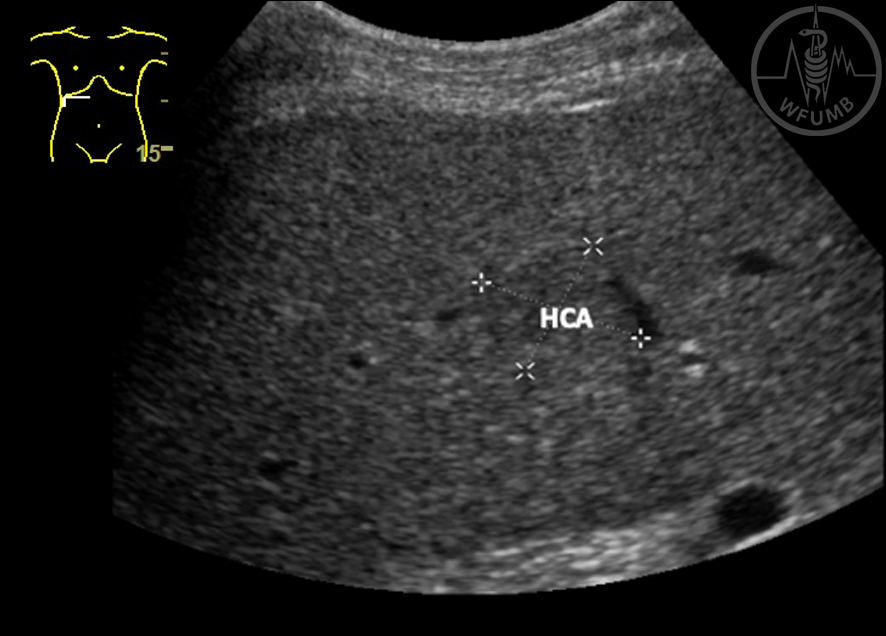
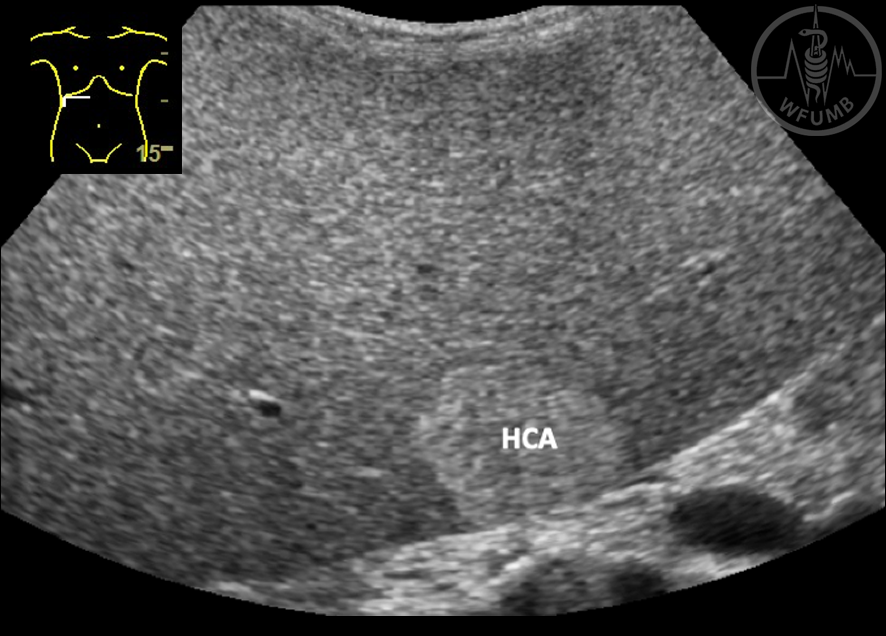
Fig 13.2.6a Hepatocellular adenoma (HCA). HCA are typically isoechoic and difficult to detect if small (histology proven HCA).
Fig 13.2.6b Hepatocellular adenoma (HCA). In patients with liver storage diseases (e.g. glycogenosis) adenomas are hyperechoic (histology proven HCA).
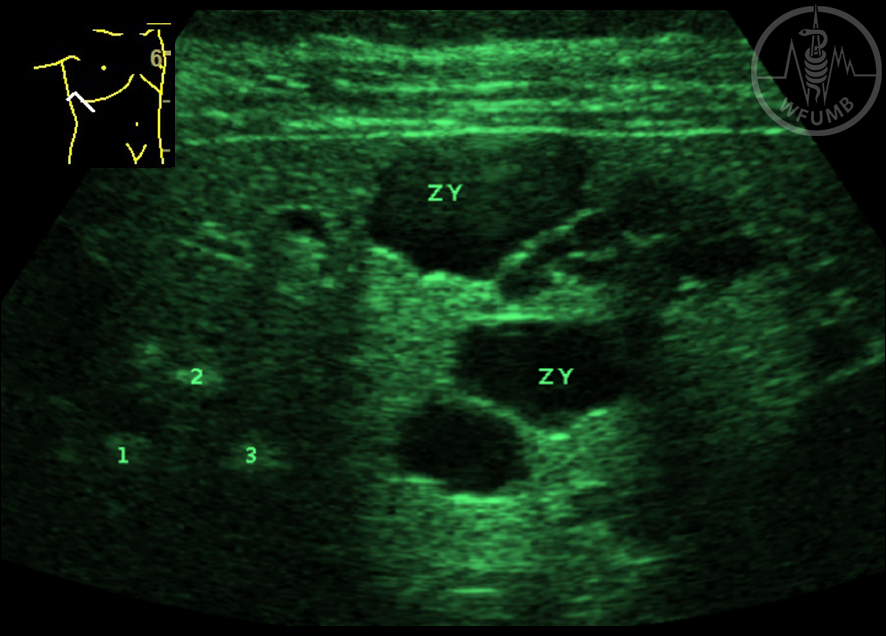
Fig 13.2.7a Biliary Hamartoma (von Meyenburg complex). Hamartomas are initially hyperechoic (when small and mostly solid) (1, 2, 3) and of mixed echogenicity with cystic components (Zy) at later stage.
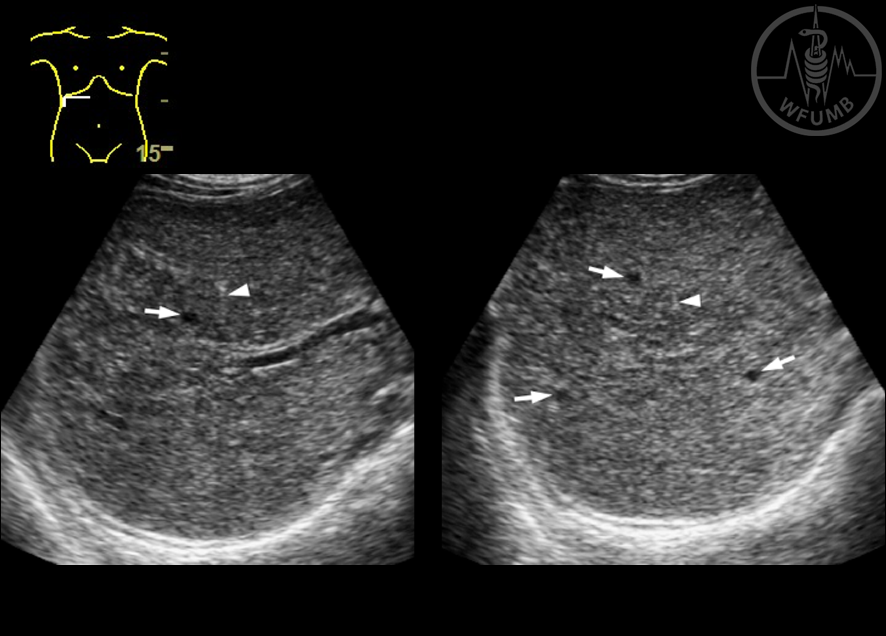
Fig 13.2.7b Biliary Hamartoma (von Meyenburg complex). Sometimes the liver parenchyma appears to be coarse and contains tiny cysts (arrows) and comet tail artefacts (arrowheads) on the ultrasound images
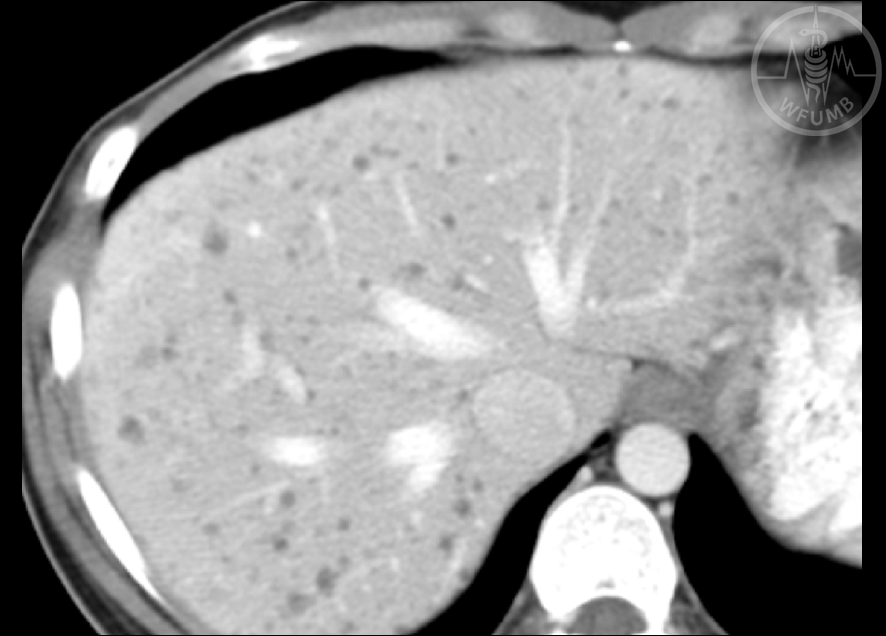
Fig 13.2.7c Biliary Hamartoma (von Meyenburg complex). Numerous tiny cysts are clearly delineated on the portal phase CT image
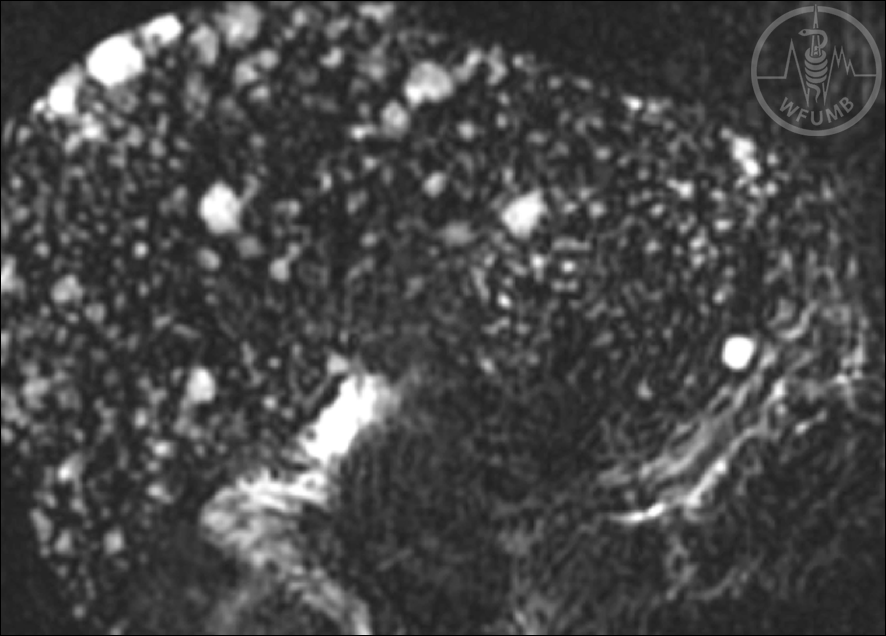
Fig 13.2.7d Biliary Hamartoma (von Meyenburg complex). Numerous tiny cysts are clearly delineated on T2-weighted coronal MR image
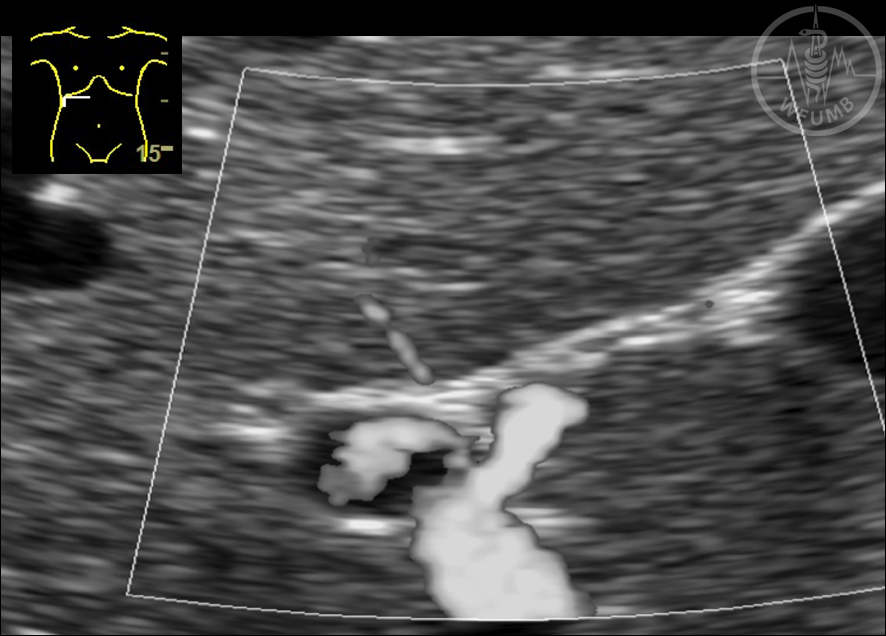
Fig 13.2.8a
Focal fatty sparing (FFS)
FFS typically shows centrally located feeding arterial vessels, with less insulin and fat concentration demonstrating the underlying pathological process of different vascularisation of the liver hilum
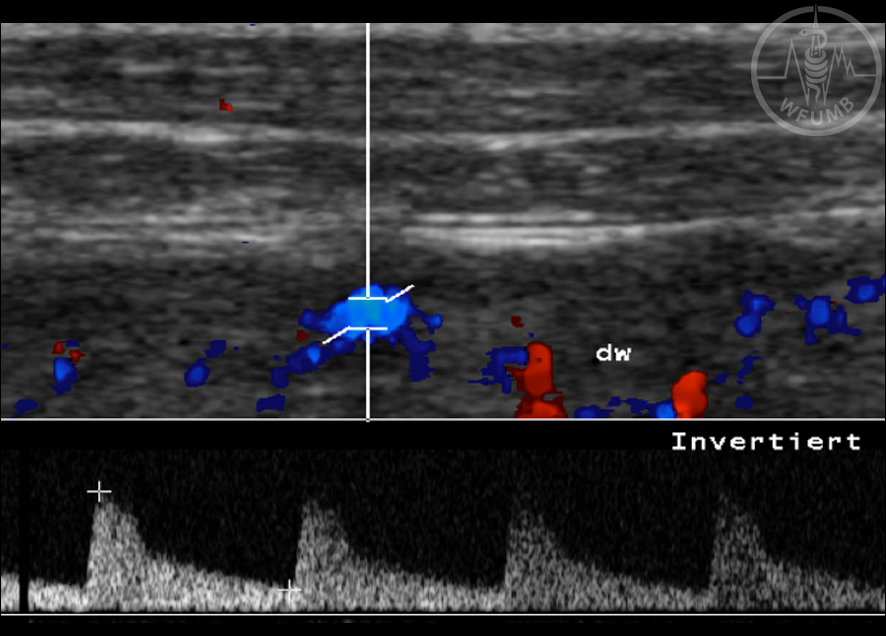
Fig 13.2.8b
Focal fatty sparing (FFS) The arterial vessels can be displayed without fatty liver and, therefore, without FFS
Fig 13.2.8e
Focal fatty sparing (FFS)
CT image in the arterial phase shows the aberrant left gastric artery (arrows) supplying the focal sparing
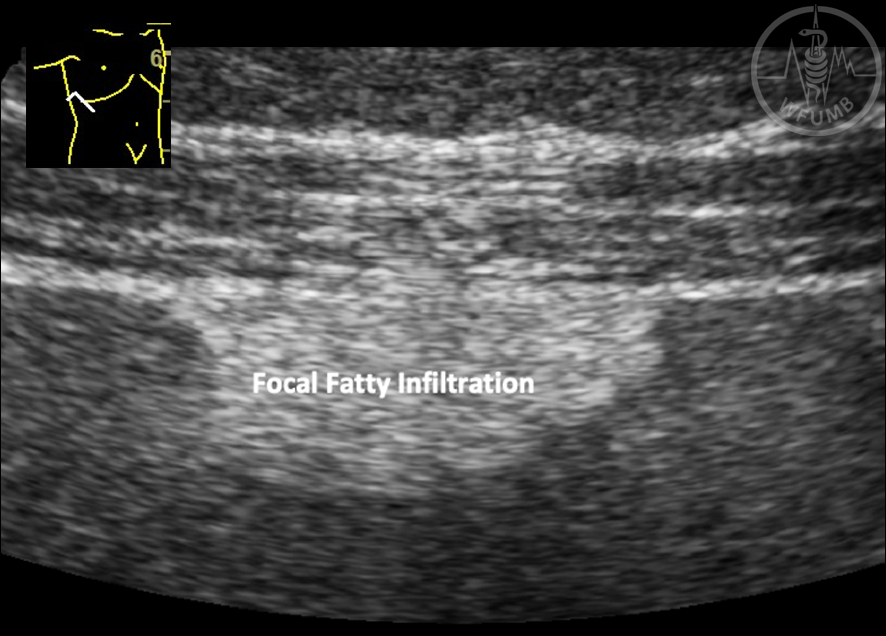
Fig 13.2.9
Focal fatty infiltration (FFI)
In FFI changes in
arterioportal venous
perfusion have been
suggested as the
pathophysiological
explanation with
predominant portal venous
flow and high content of
insulin and fat)
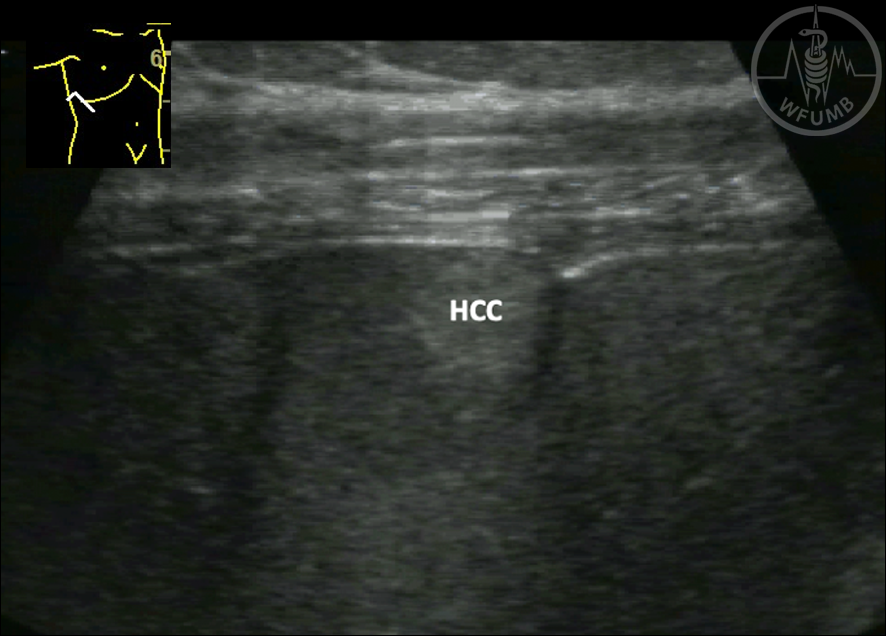
Fig 13.2.10a
Hepatocellular carcinoma
(HCC). HCC might be hyperechoic, especially when small
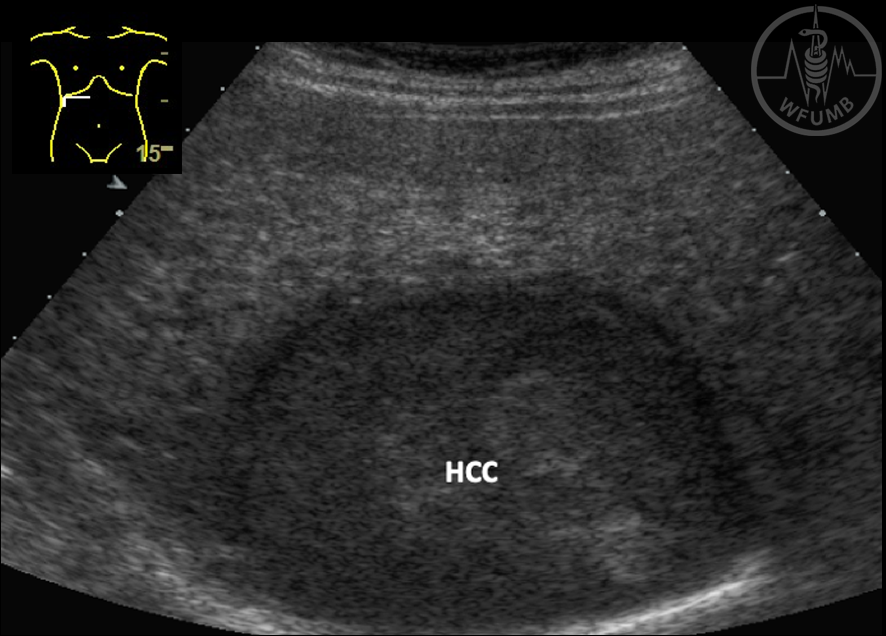
Fig 13.2.10b
Hepatocellular carcinoma
(HCC). HCC are typically hypoechoic
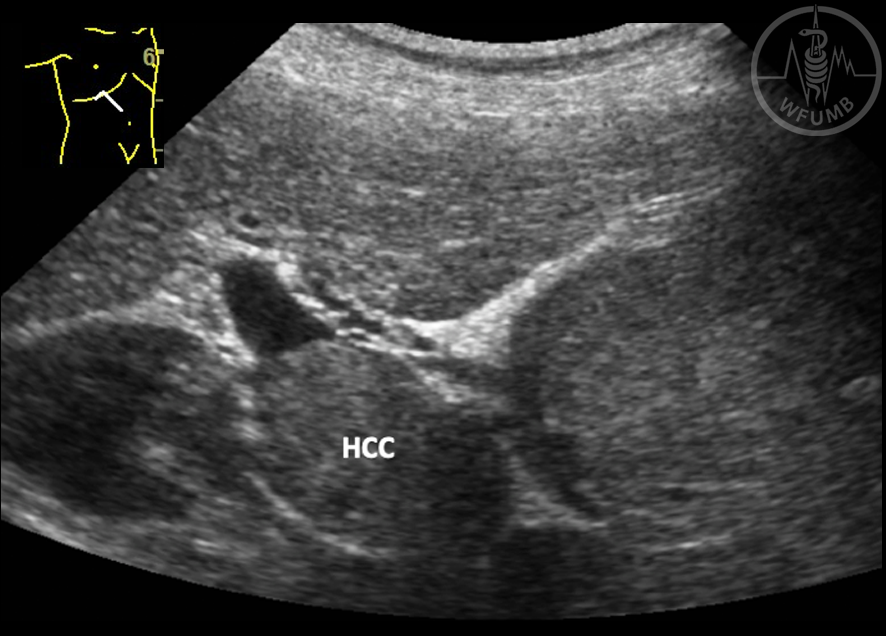
Fig 13.2.10c
Hepatocellular carcinoma
(HCC). HCC show portal vein infiltration in up to 25 % of non-screened patients
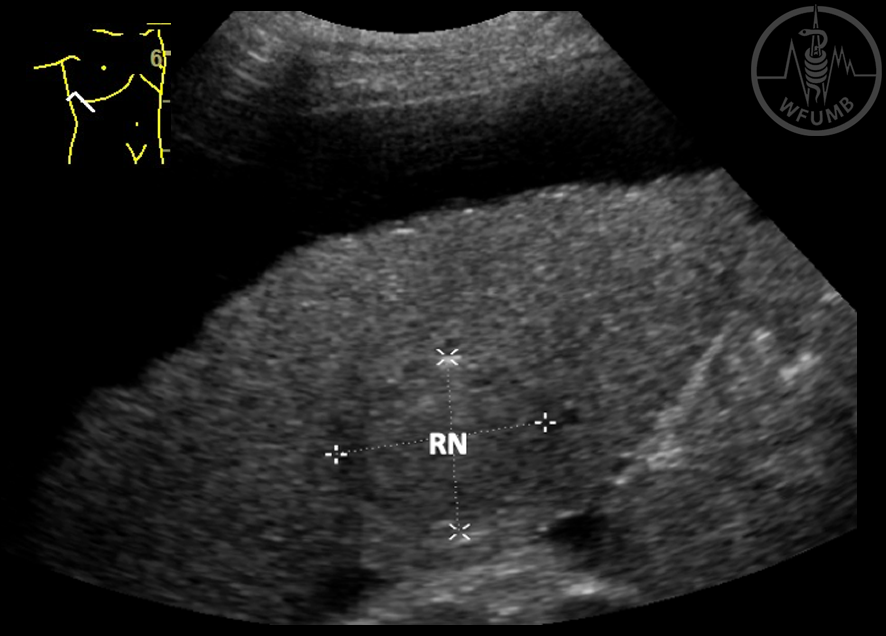
Fig 13.2.10d
Hepatocellular carcinoma
(HCC). Regenerative nodules (RN) might show a size up to 35 mm.
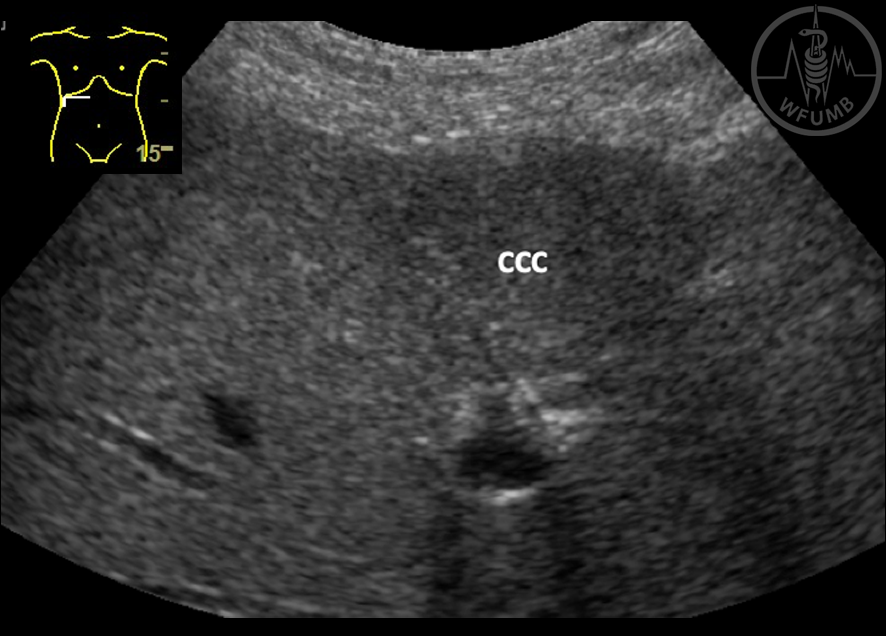
Fig 13.2.11
Cholangiocarcinoma (CCC). Peripherally located CCC, slightly hypoechoic with satellite metastases (at surgery)
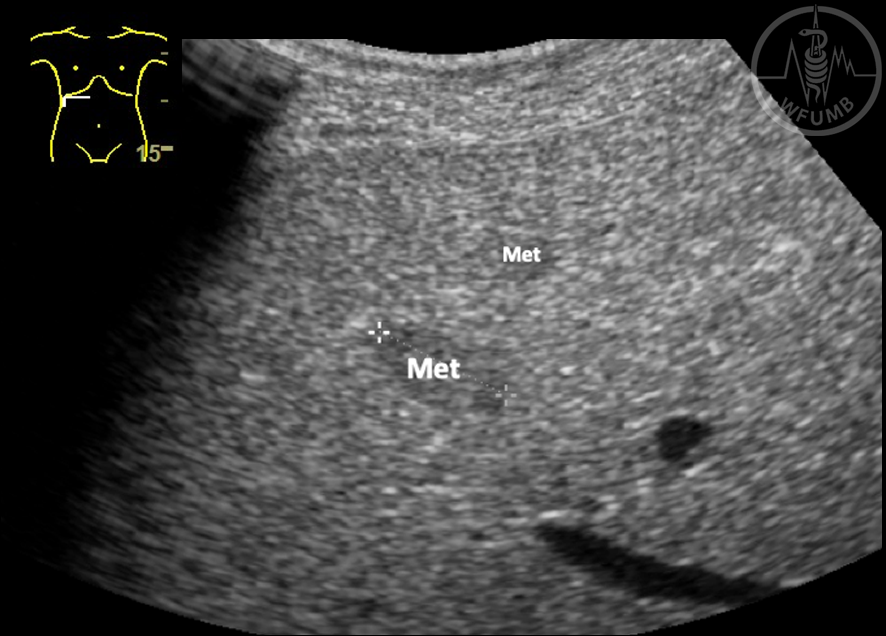
Fig 13.2.12a
Metastases. Metastases might be small and iso- or slightly hypoechoic and difficult to detect
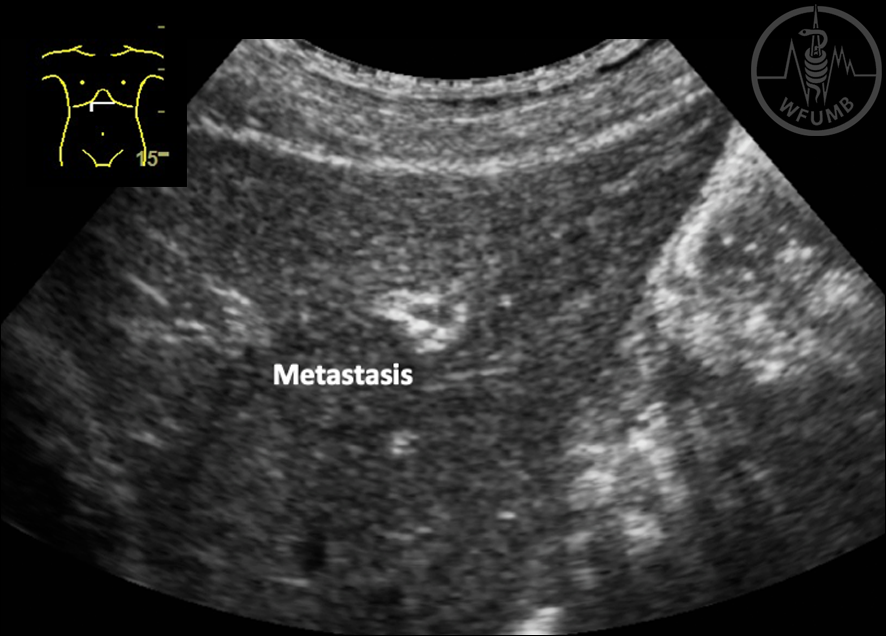
Fig 13.2.12b
Metastases. Metastases might be small and iso- or slightly hypoechoic and difficult to detect
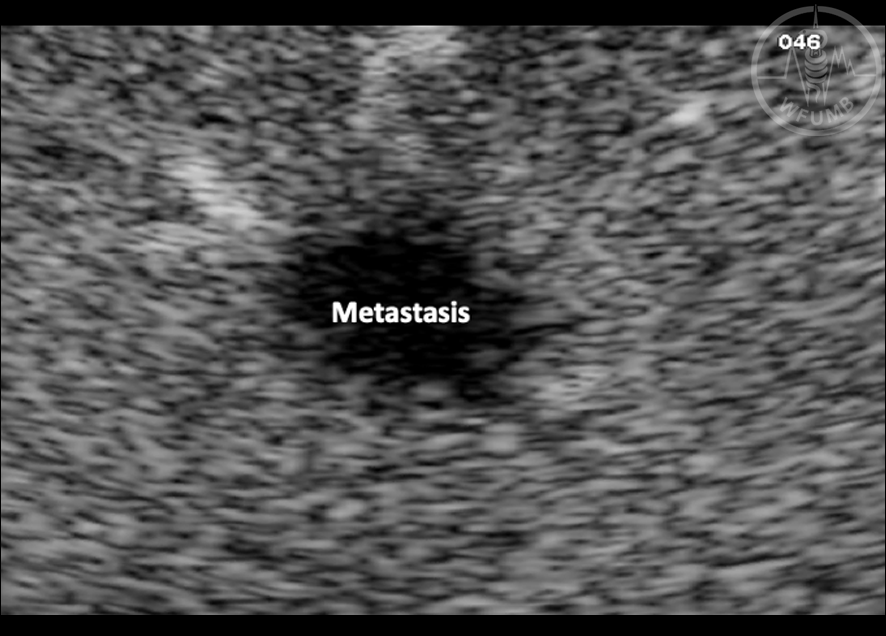
Fig 13.2.12c
Metastases. Necrotic and larger metastases tend to be hypoechoic. Hyperechoic metastases may occur as well
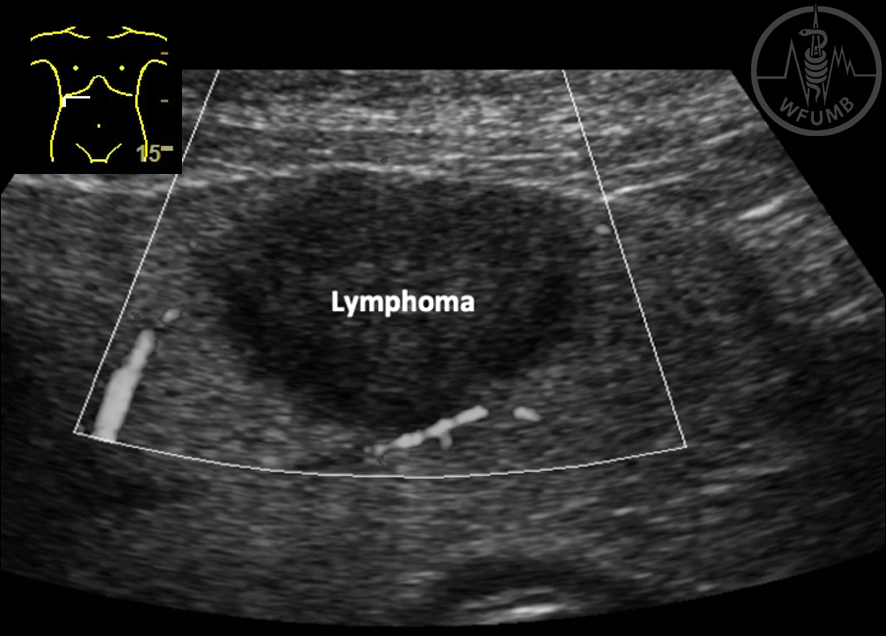
Fig 13.2.13
Lymphoma. Circumscribed lymphomas can infiltrate the liver in small or large nodules or over an extended area, and depending on their rate of growth, are often very hypoechoic compared with the surrounding liver tissue
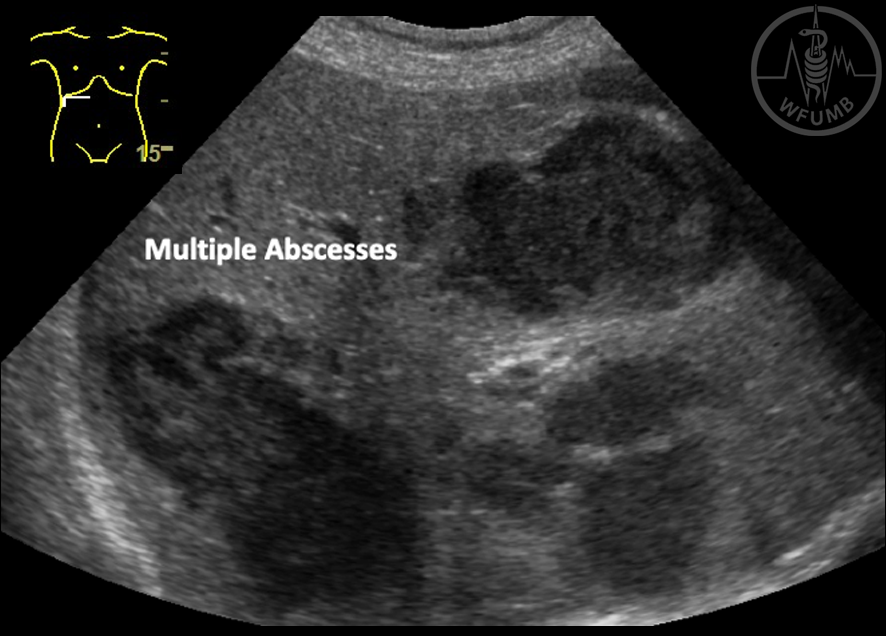
Fig 13.2.14
Abscess. The patient’s medical history and occasionally the physical examination (pyrexia or signs of sepsis) are the most helpful in differentiating abscesses from necrotic metastases
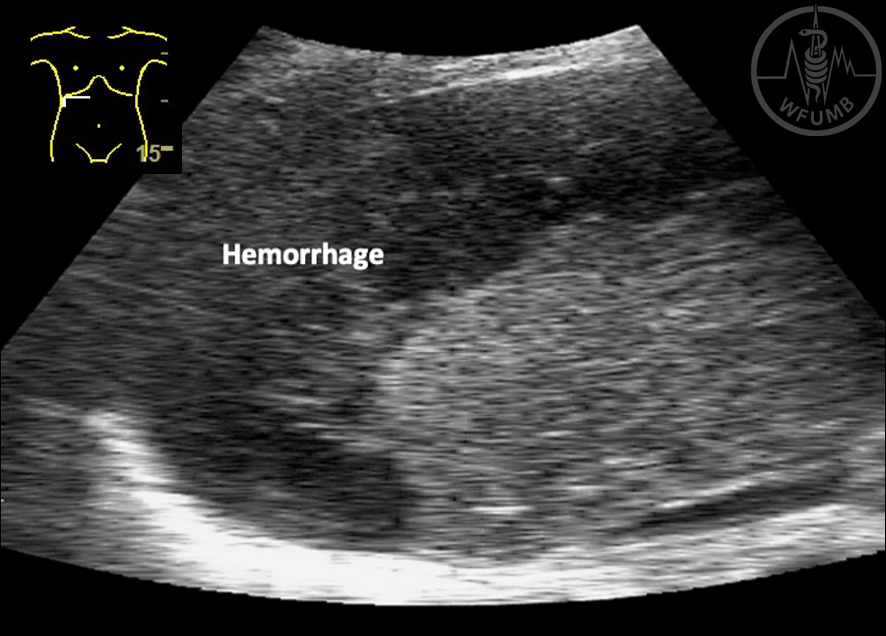
Fig 13.2.15
Hemorrhage.
The spontaneously evolving and painful haematoma is typical for amyloidosis of the liver
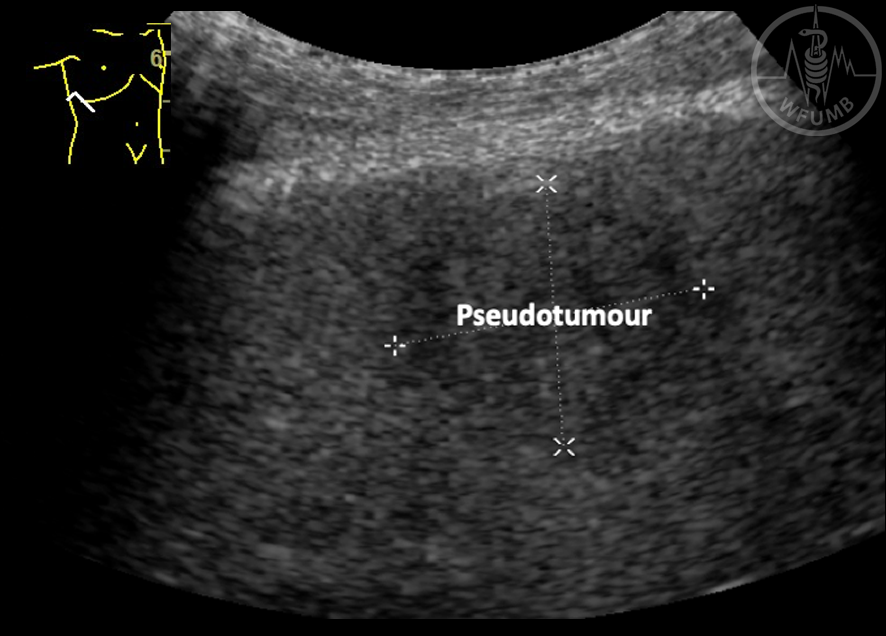
Fig 13.2.16
Inflammatory pseudotumour. The definitive diagnosis is only achieved by surgery (wedge resection)