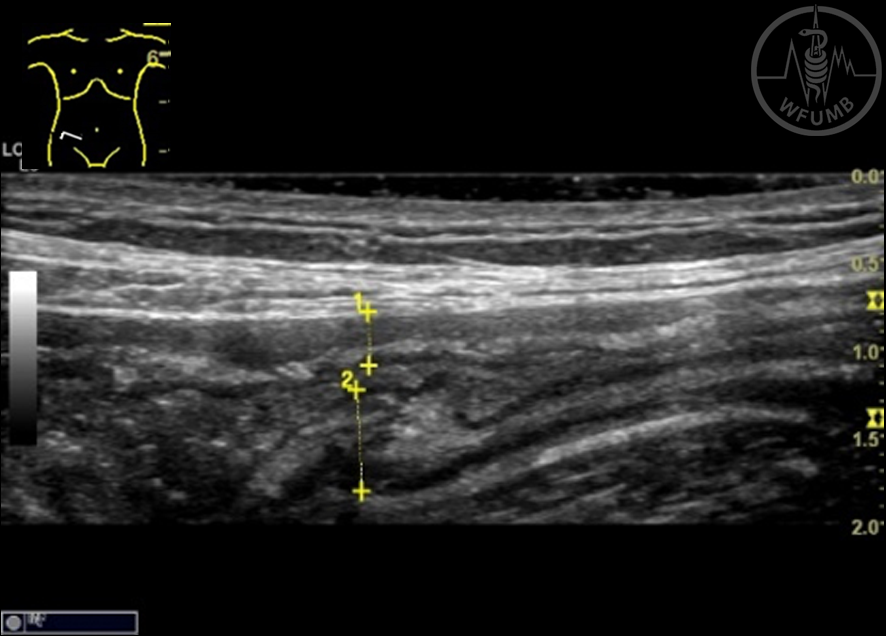
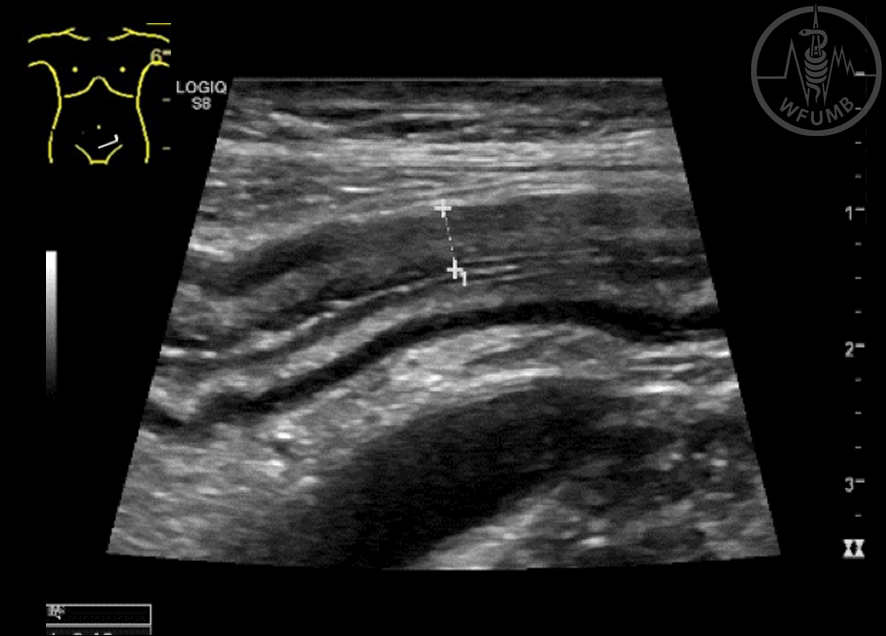
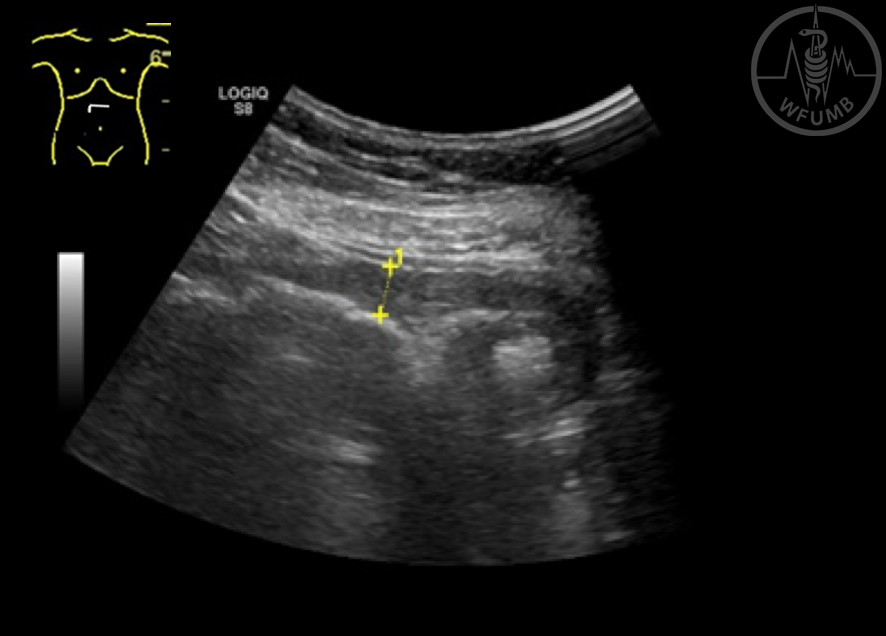
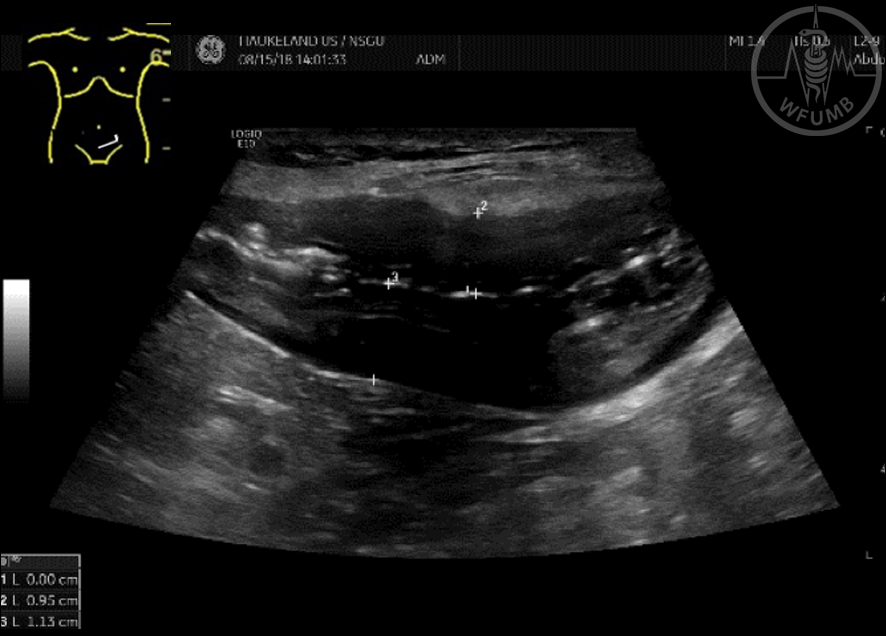
Fig 19.1a
Bowel wall thickening in Crohn’s disease. Slight wall thickening of the wall in the terminal ileum in a patient with mild disease
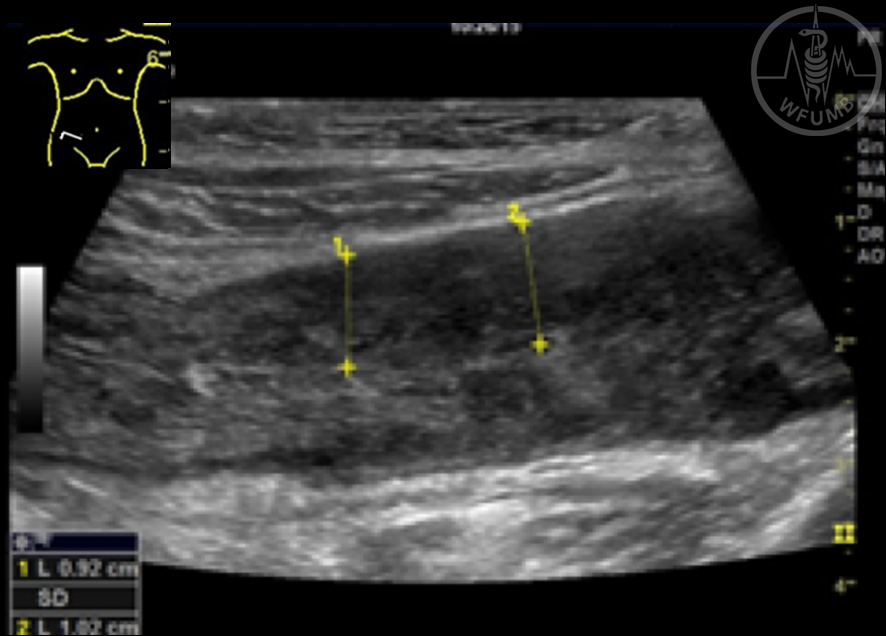
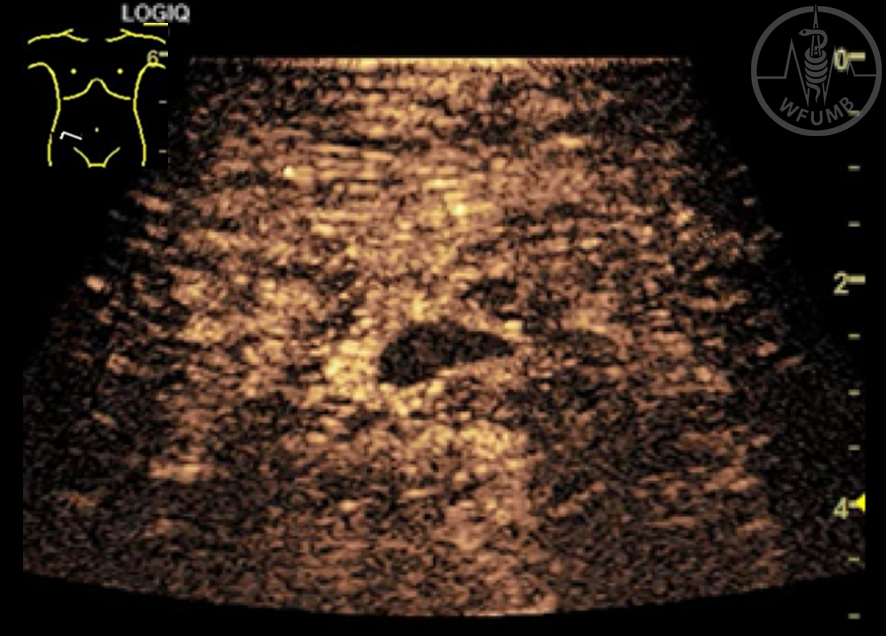
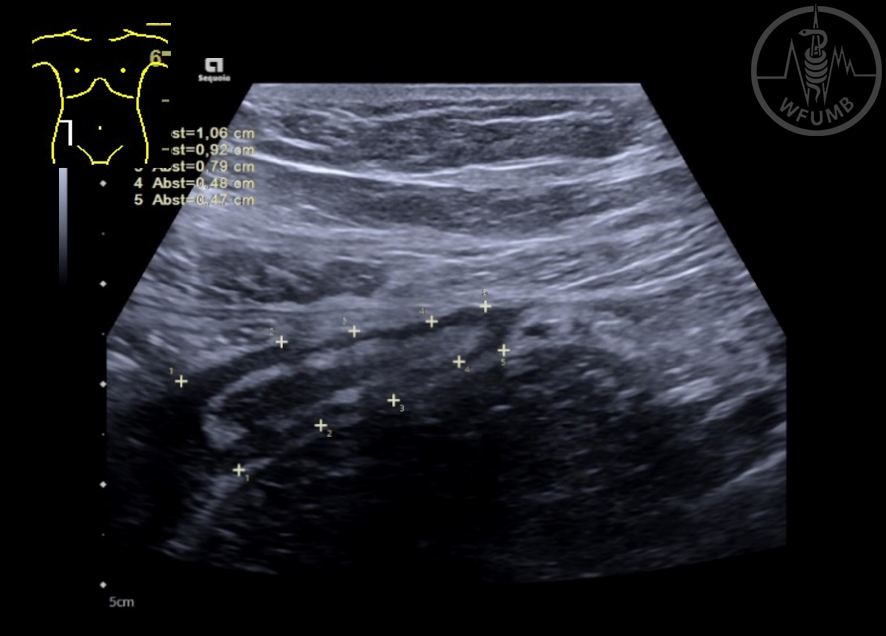
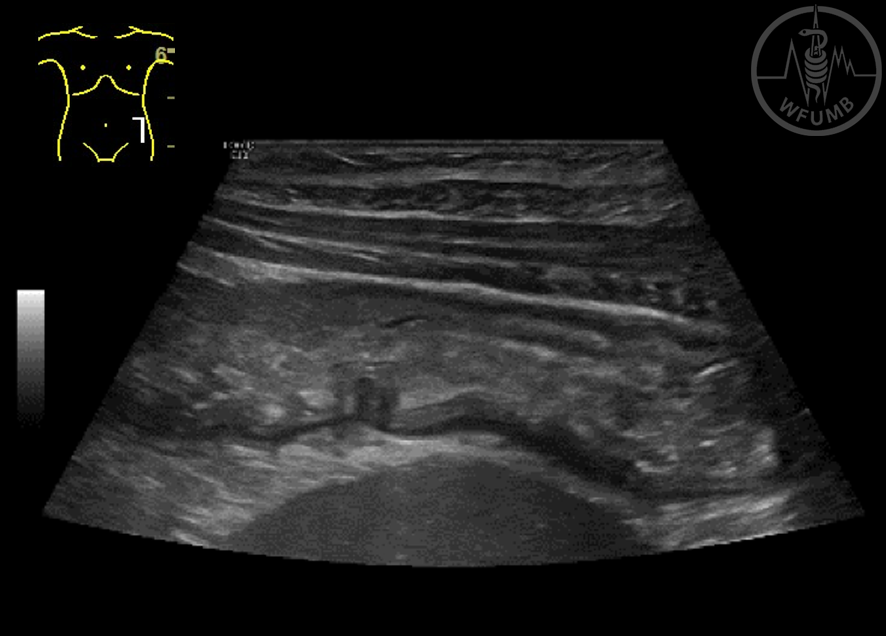
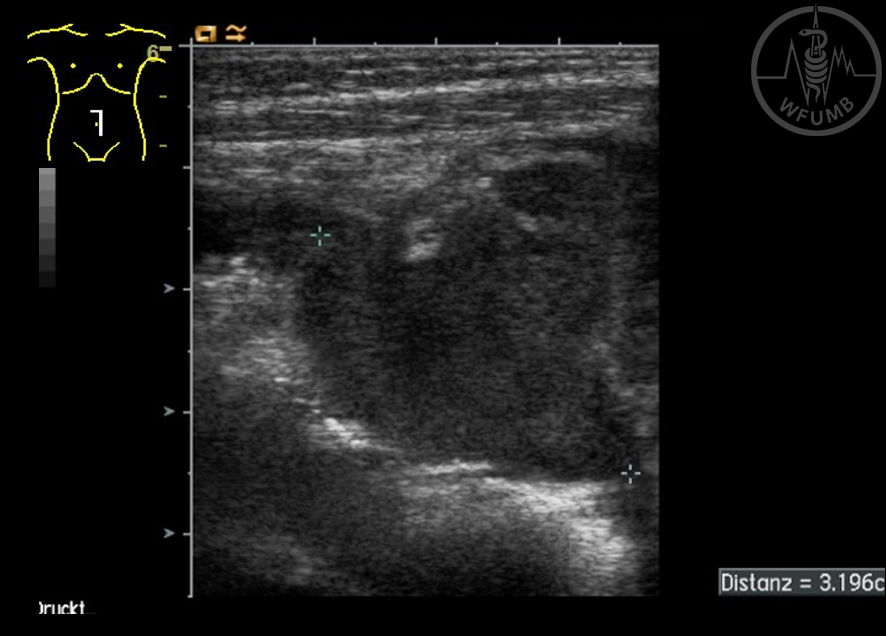
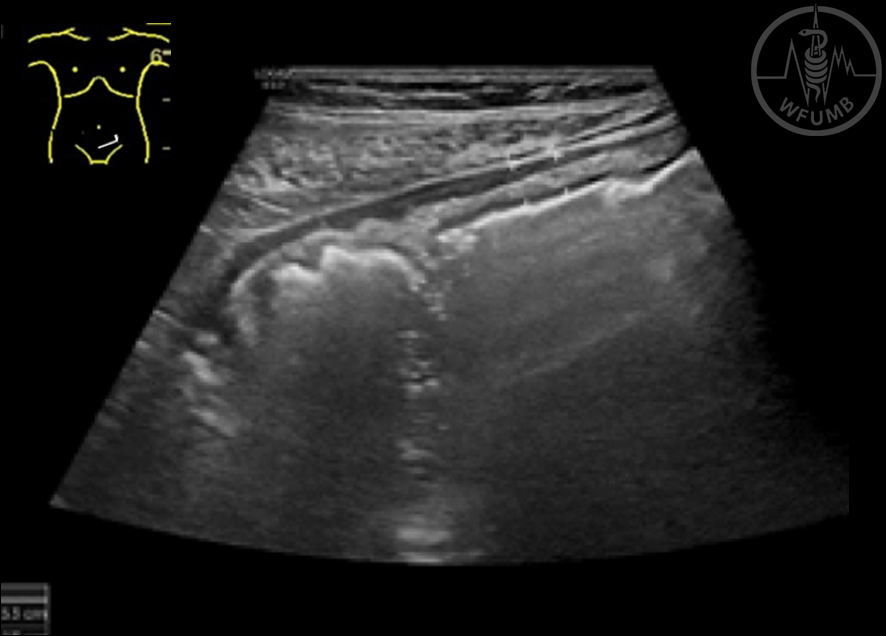
Fig 19.1b
Bowel wall thickening in Crohn’s disease. Gross thickening of the bowel wall with loss of wall layers in a patient with severe disease
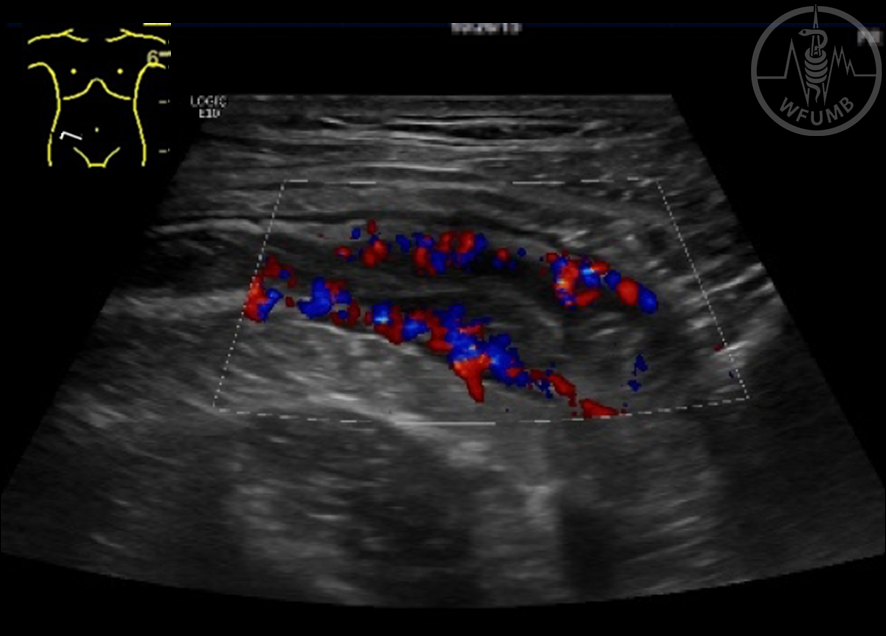
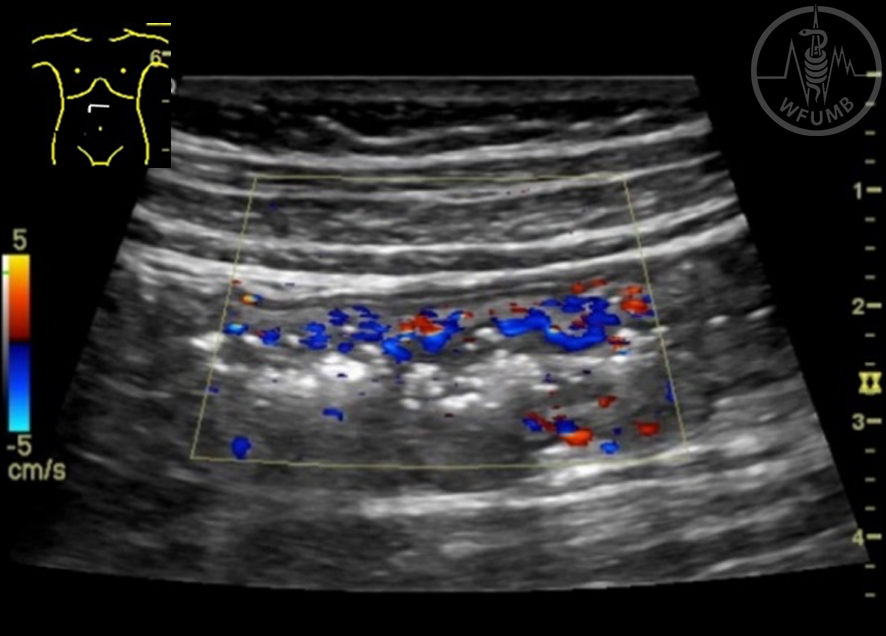
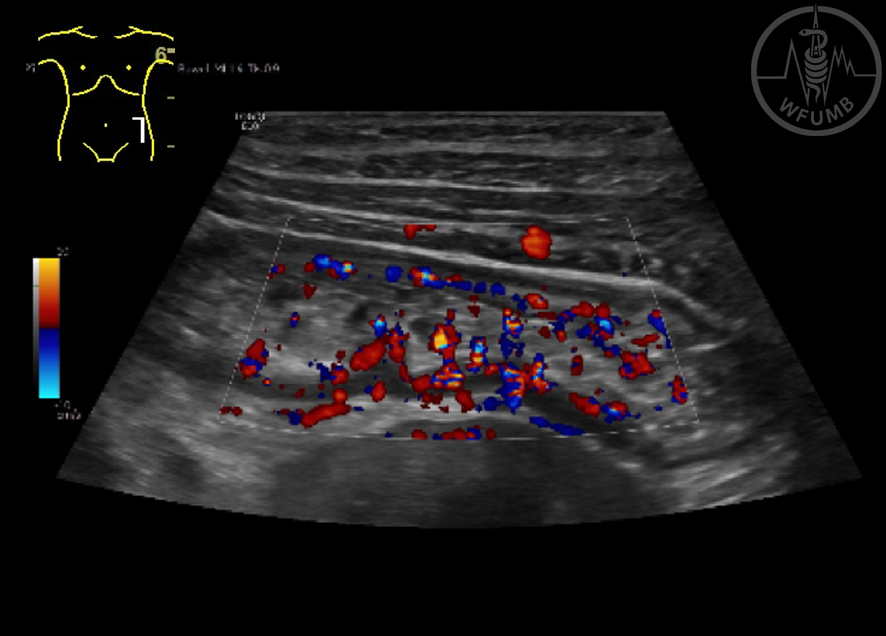
Fig 19.1c
In active Crohn’s disease multiple dilated vessels can be seen inside the bowel wall using colour Doppler
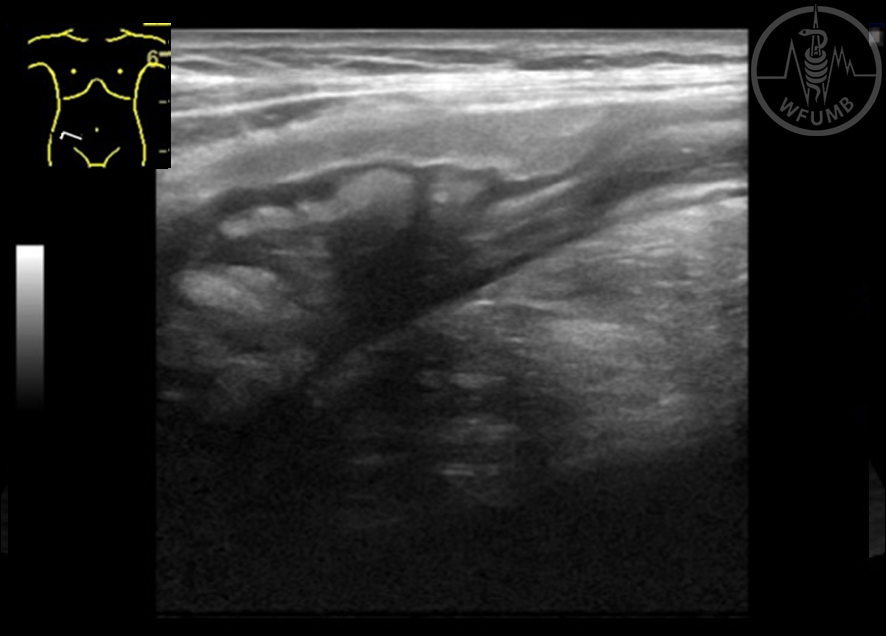
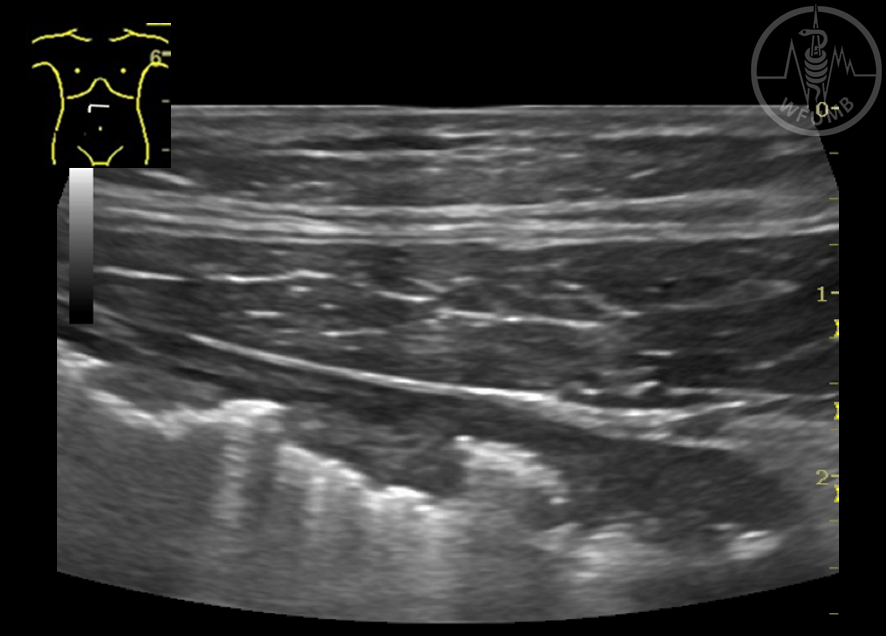
Fig 19.1d
Fatty wrapping is a typical finding in Crohn’s disease and is typically hyperechoic. Here it is seen encircling a chronically inflamed terminal ileum
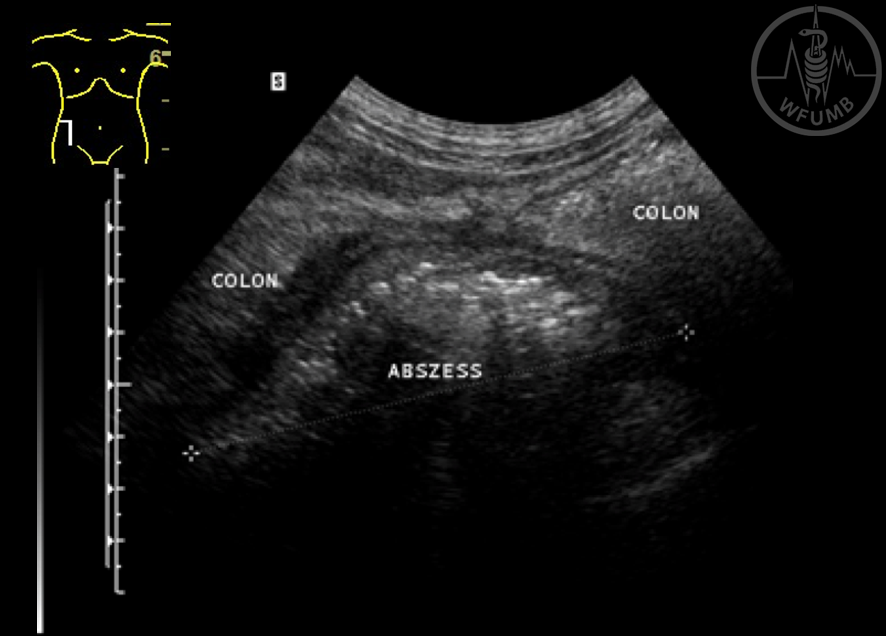
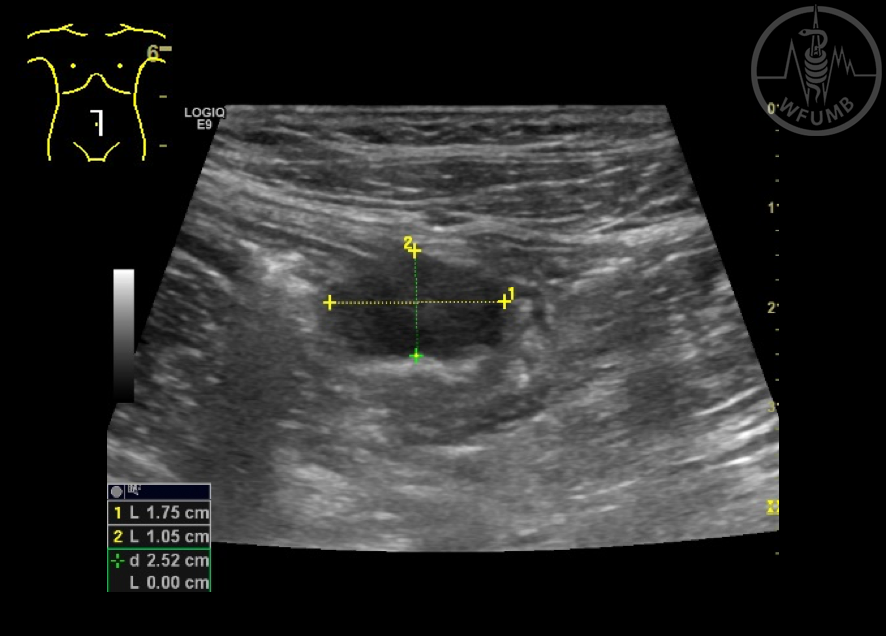
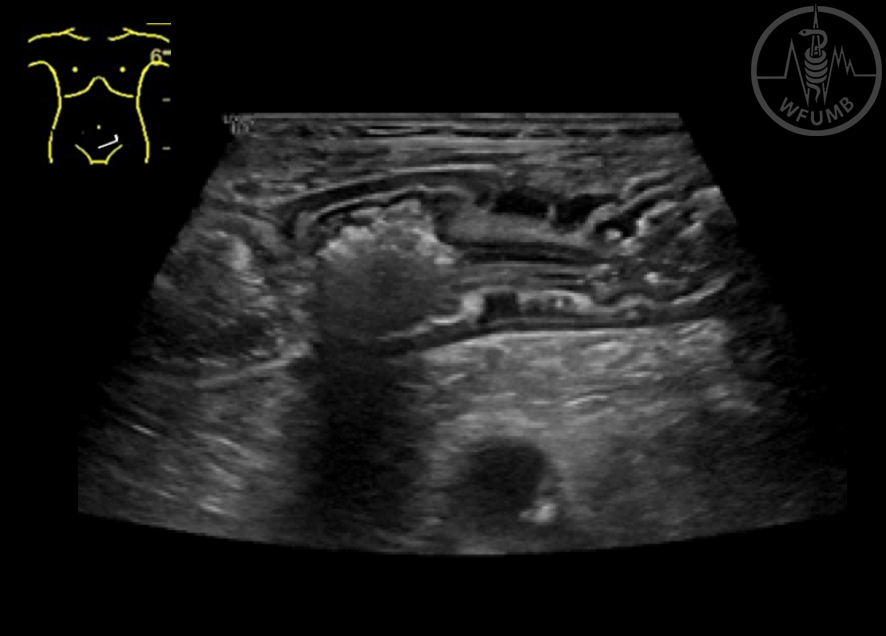
Fig 19.2a
Crohn’s disease complications. Abscess in association with an inflamed small bowel loop central in the abdomen
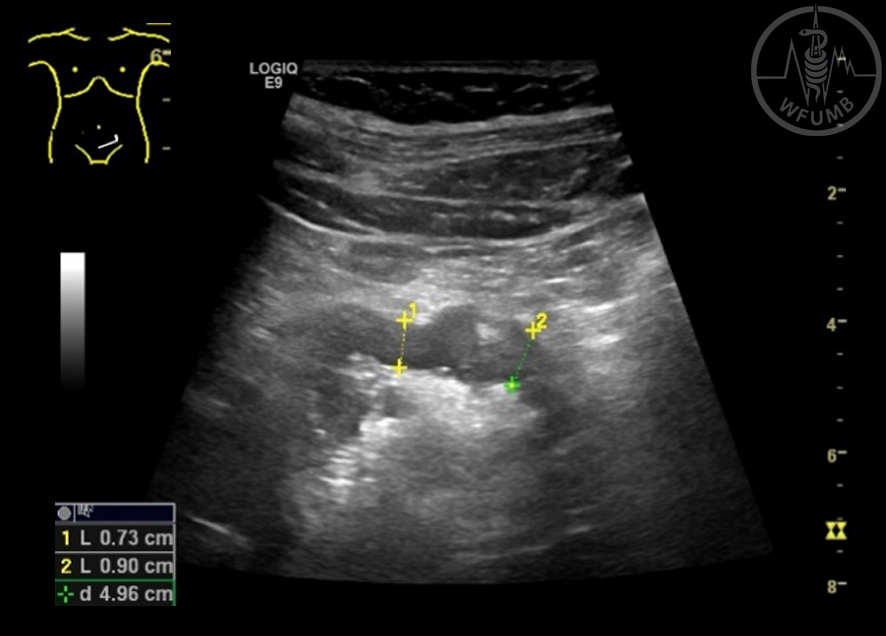
Fig 19.2b
Crohn’s disease complications. A fistula tract can be seen going out from affected terminal ileum going into an abscess behind the urinary bladder
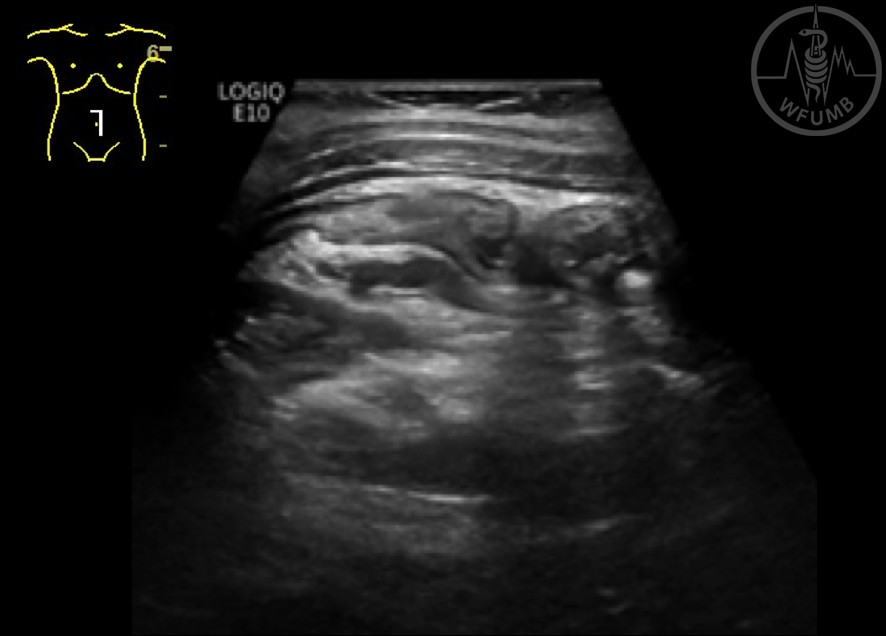
Fig 19.2c
Crohn’s disease complications. A stenosis in the terminal ileum is shown with the transition to normal wall thickness
Fig 19.2d
Crohn’s disease complications. The ultrasonogram shows grossly dilated intestinal loop just prior to the stenosis in Crohn’s disease
Fig 19.3a
Using ultrasound contrast you can separate and infiltrate from an abscess. In this case the B-mode image shows and infiltrate in relation to inflamed small bowel
Fig 19.3b
Using ultrasound contrast you can separate and infiltrate from an abscess.
In the contrast image a small abscess in the central part of the infiltrate is seen as a perfusion defect
Fig 19.4a
Mild ulcerative colitis
Fig 19.4b
Severe ulcerative colitis. Note the destruction of wall layers
Fig 19.4c
Colour Doppler reveals multiple dilated vessels inside the inflamed transverse colon in patient with active ulcerative colitis
Fig 19.4d
Be aware that pseudo-polyps can cause a thickening of the bowel wall. Here seen in the transverse colon in a patient with quiescent disease. Between the polyps, normal wall with retained stratification can be seen
Fig 19.5
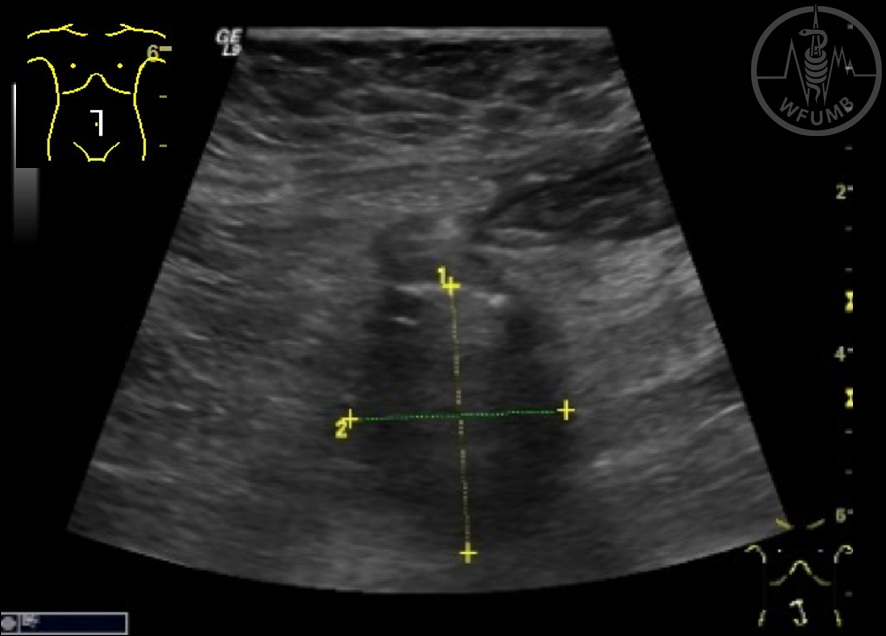
Thickened, inflamed appendix is shown
Fig 19.6
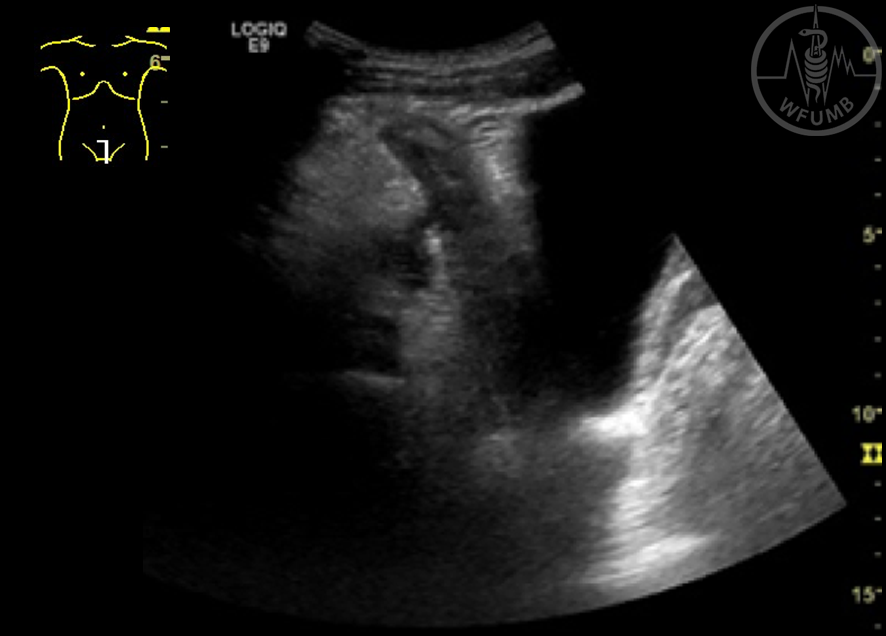
In a patient with six weeks history of fever, abdominal pain and painful walking in the last days, a retrocecal abscess can be seen in a patient with perforated appendicitis
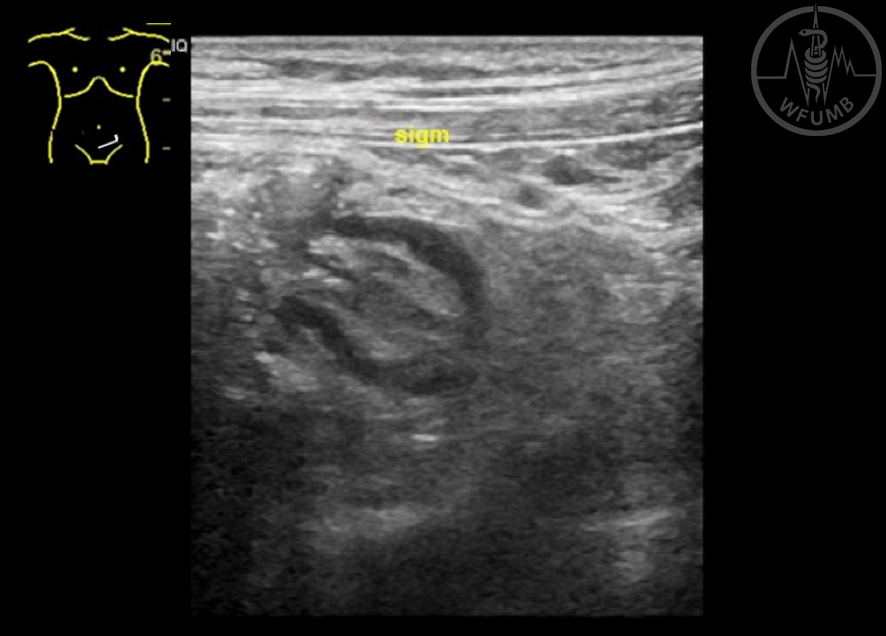
Fig 19.7
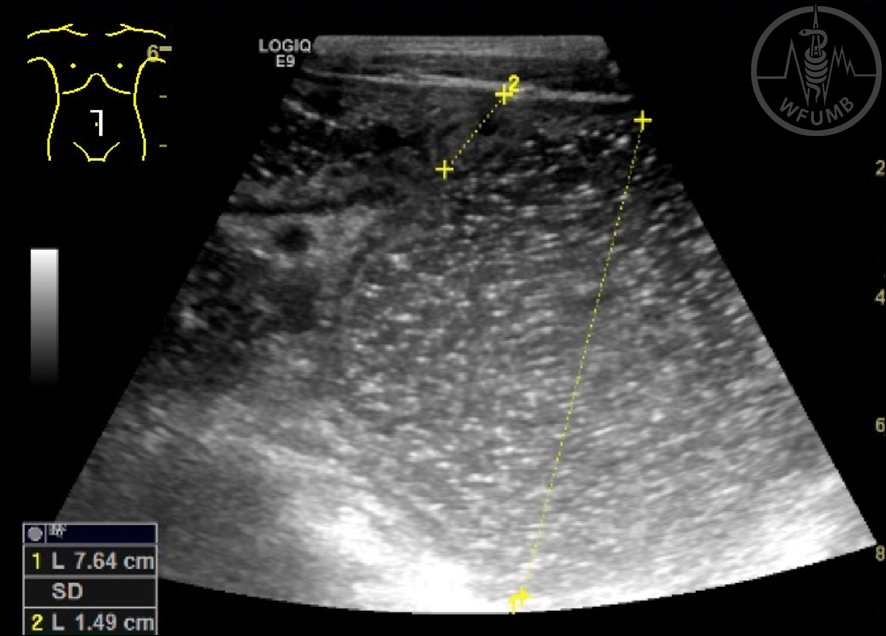
An inflamed diverticula with a thickened hypoechoic wall and with hyperechoic content can be seen originating from sigmoid colon
Fig 19.8a
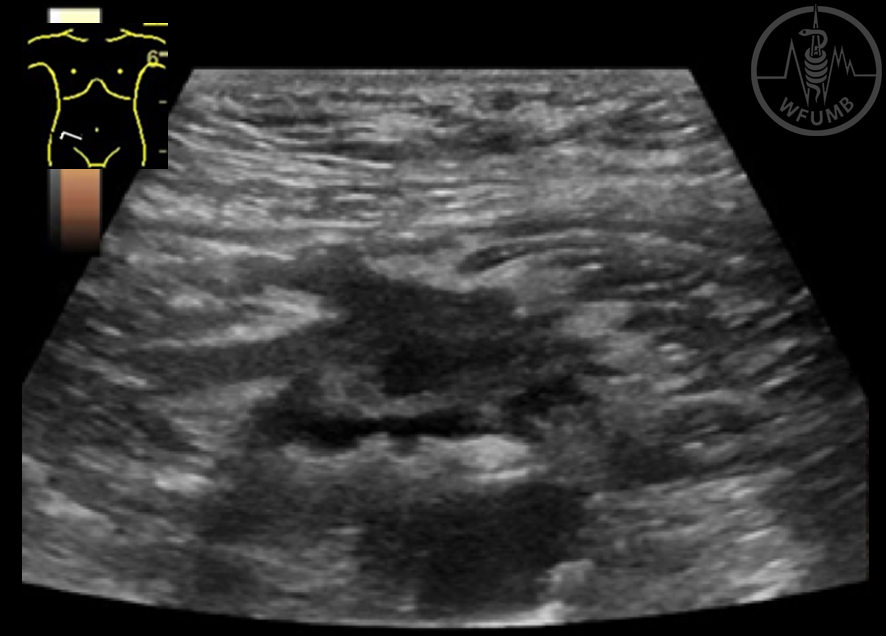
A patient with abdominal pain and vomiting had dilated small bowel
Fig 19.8b
A patient with abdominal pain and vomiting had dilated small bowel and a femoral hernia was revealed as the cause
Fig 19.9a
Often a patient with ischemic colitis is examined in the reperfusion phase of ischemic colitis.
Edematous wall with a slight loss of stratification
Fig 19.9b
Often a patient with ischemic colitis is examined in the reperfusion phase of ischemic colitis. With colour Doppler plenty of dilated vessels can be found
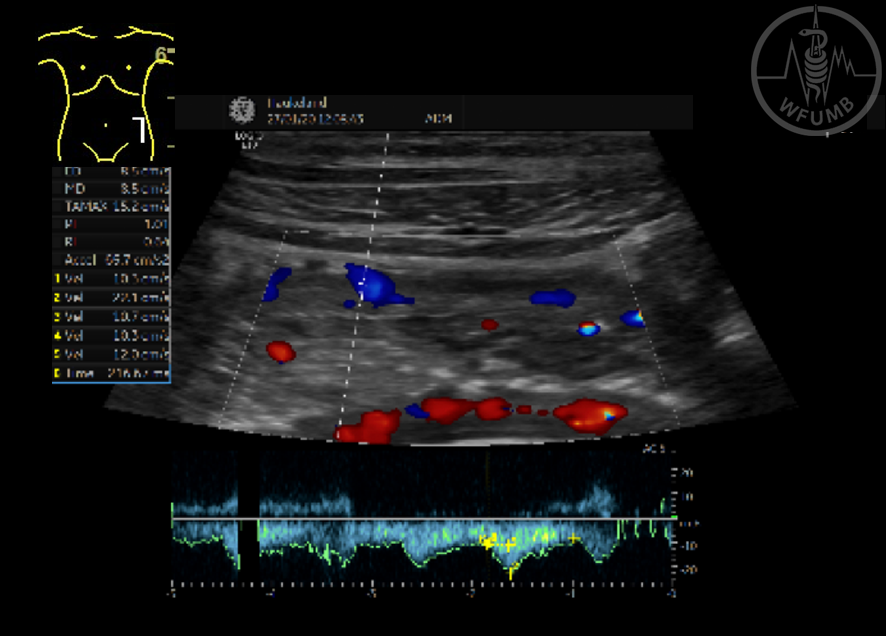
Fig 19.9c
Often a patient with ischemic colitis is examined in the reperfusion phase of ischemic colitis. By adding pulse wave Doppler in intramural arteries, typically a delayed acceleration time can be detected
Fig 19.10
A grossly thickened gastric wall with loss of wall layers can be found in patients with linitis plastica
Fig 19.11
Burkitt’s lymphoma in the gastrointestinal tract
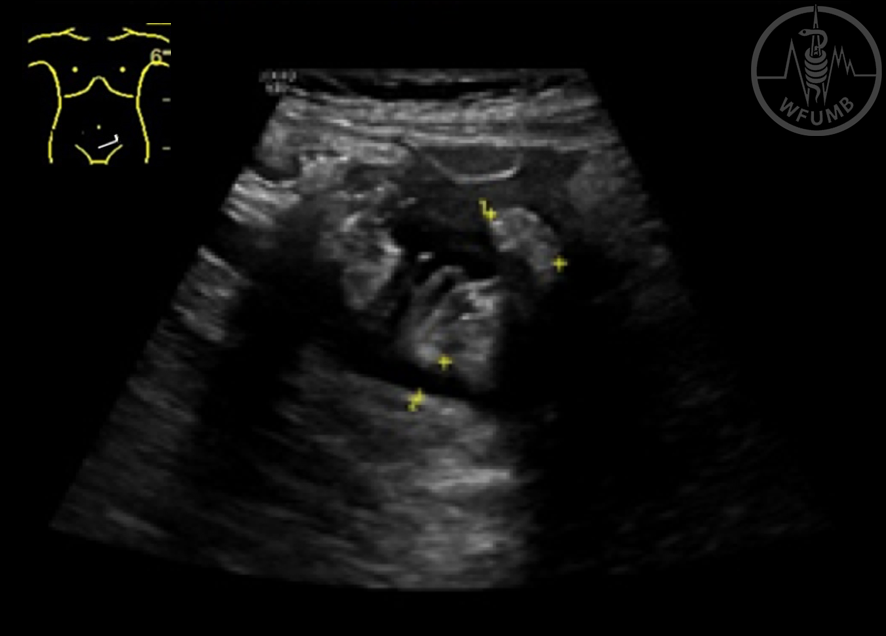
Fig 19.12a
GIST. In a patient with abdominal pain and episodes of subileus, a hypoechoic, rounded mass was found in the wall of a small bowel segment. The tumour compressed the lumen causing symptoms and could be seen emerging from the proper muscle layer.
Fig 19.12b
GIST. Just nearby a round lymph node was found in the mesentery. The patient was operated and histology confirmed a GIST with lymph node metastasis.
Fig 19.13
Neuroendocrine tumour located in the mesenterium
Fig 19.14a
Typical “pseudo-kidney” sign is seen in a patient with colon cancer
Fig 19.14b
A stricturing tumour of the sigmoid colon
Fig 19.15a
Image from acute GVHD of the colon. Grossly thickened bowel wall is shown with extra hyperechoic lines towards the lumen representing the sloughing off of the mucosa
Fig 19.15b
Image from acute GVHD of the colon. Hyperaemia with colour Doppler
Fig 19.15c
Image from chronic GVHD of the colon. The colonic wall is shown after 4 months. The stratification is clear, but still the submucosa is thickened
Fig 19.15d
Image from chronic GVHD of the colon. The sigmoid colon is shown thickened, stiff and stenotic. The luminal content is still fluid like even though we are in the distal part of the colon
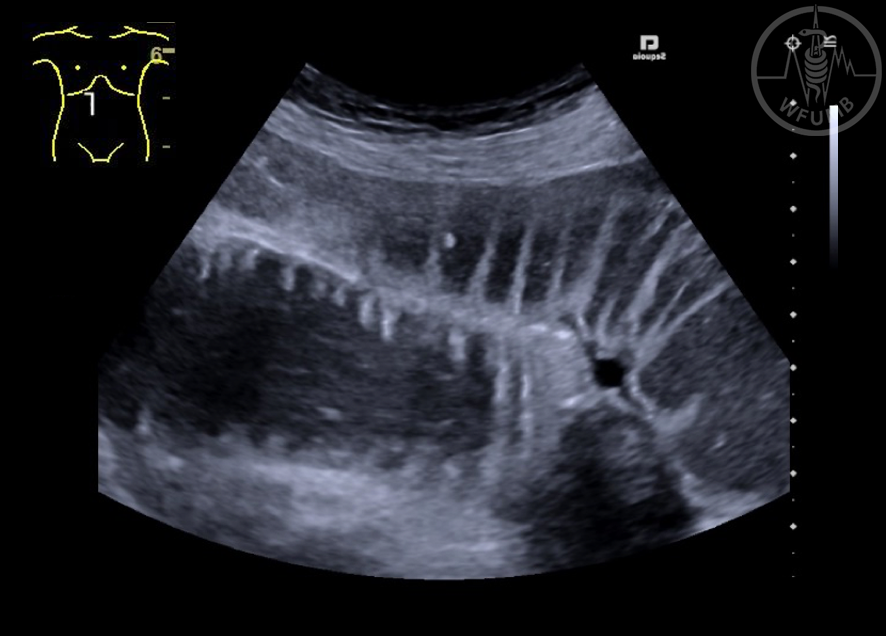
Fig 19.16a
The image shows a classical “onion sign” in a young female patient with invagination. The patient was operated and invagination due to a polyp was confirmed. The polyp can be seen as a dark greyish “sausage” in the center of the invaginate together with mesentery in white
Fig 19.16b
A longitudinal view from a patient with large polyps causing the invagination. In this section the mesentery can be seen on both sides of the invaginated bowel loop on the left side of the image