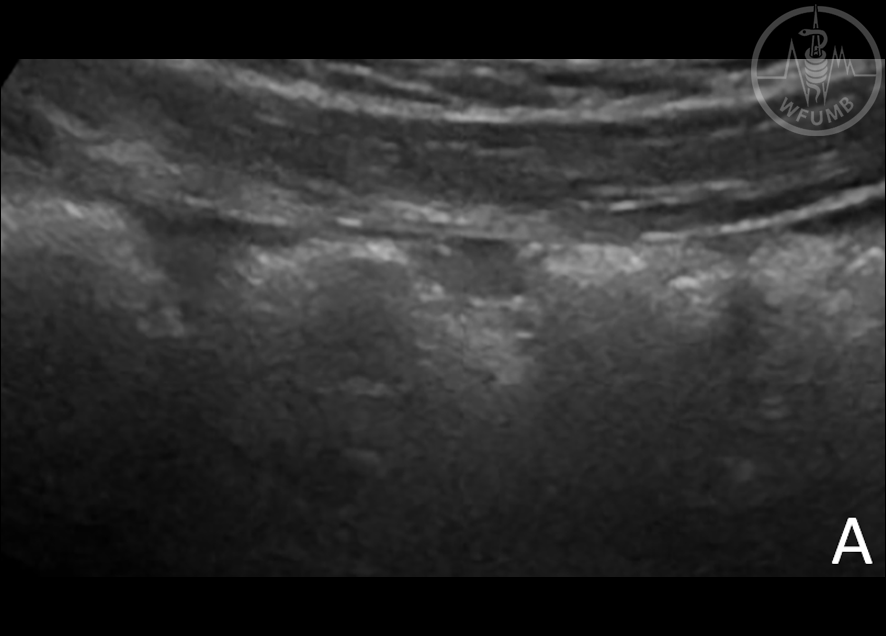
Fig 12.1a
A head-to-head comparison between low- and high-frequency transducers.
The images are obtained from the ascending colon. In panel A, a sonographic image using low frequency is depicted (5 MHz)
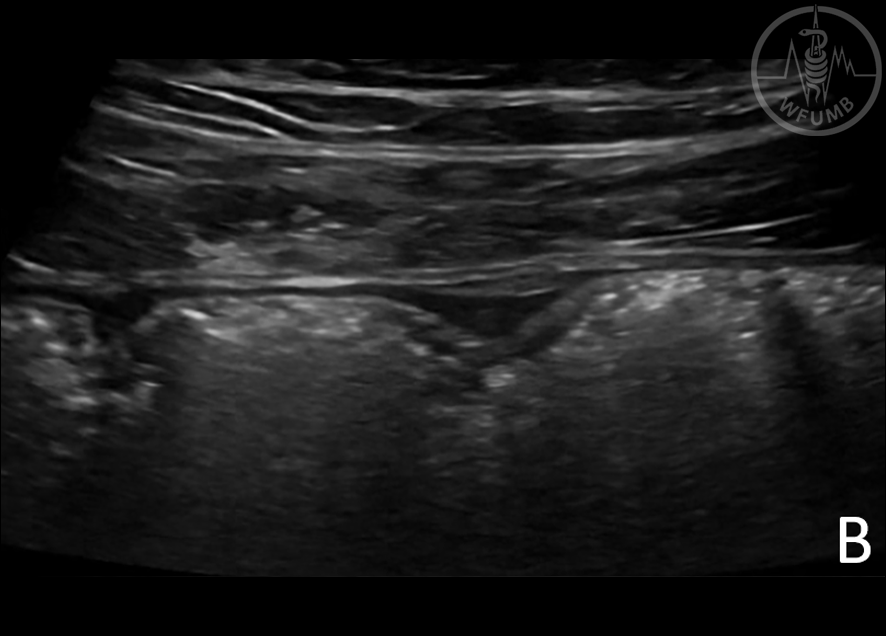
Fig 12.1b
In panel B, a high-frequency transducer (9 MHz) is used allowing for a better delineation of bowel wall layers
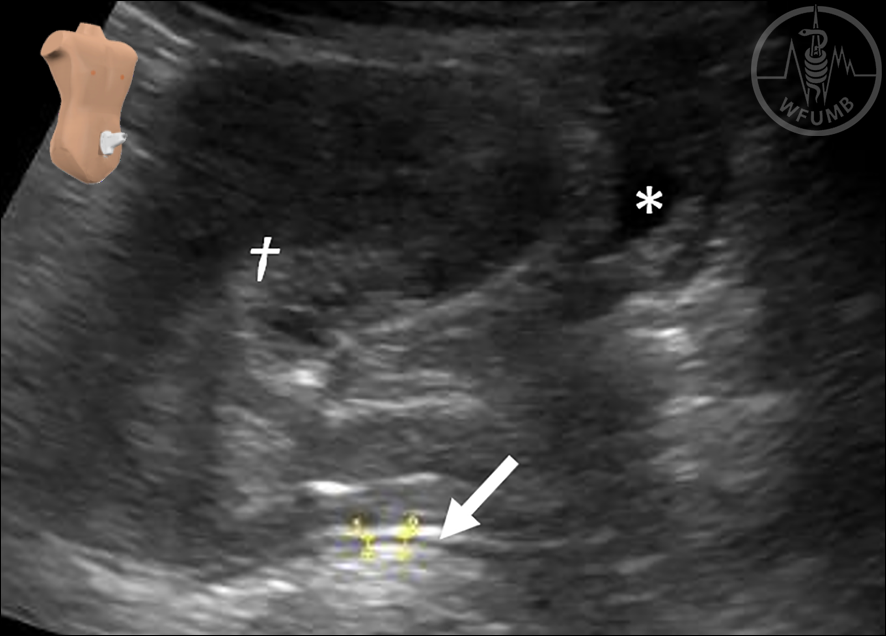
Fig 12.2
The rectum (arrow) can be identified beyond the urinary bladder (asterisk) and genitals (cross). A low-frequency transducer is usually required as the bowel segment is deeply located
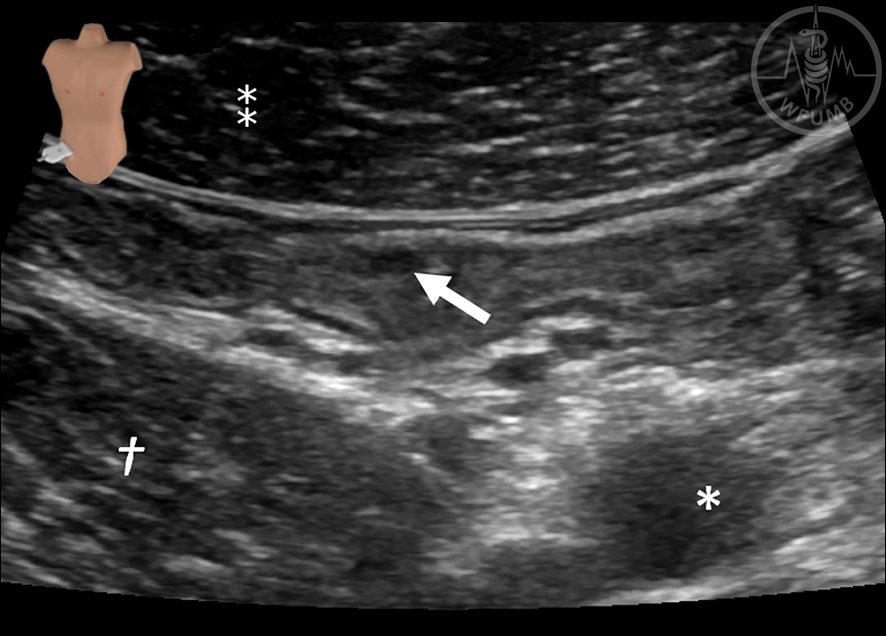
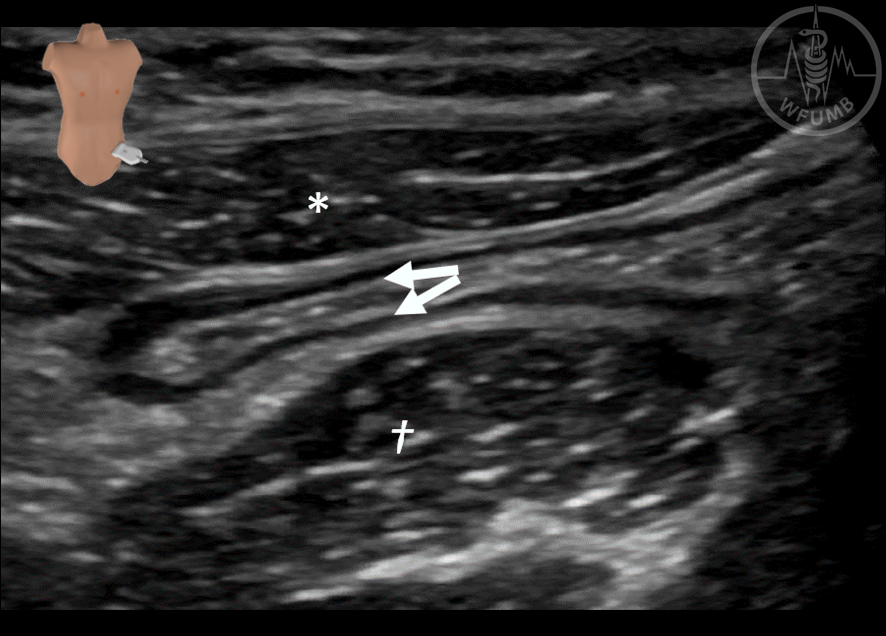
Fig 12.3
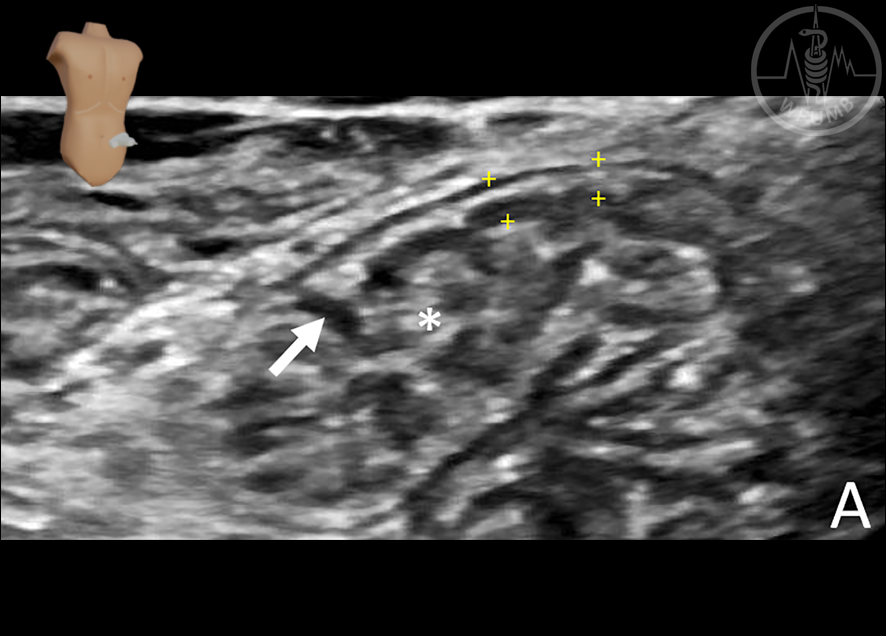
The terminal ileum (arrow) is located in the right fossa, positioned between the abdominal wall (double asterisk) and the iliopsoas muscle (cross). The terminal ileum crosses medial-to-lateral of the right iliac vessels (asterisk), making these vessels important landmarks when identifying the bowel loop.
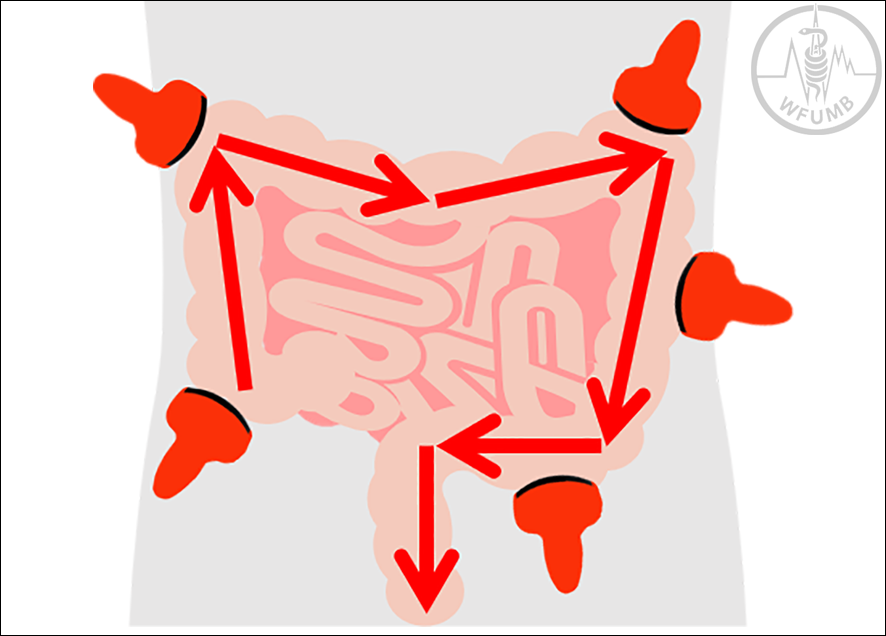
Fig 12.4
Examination technique of the large bowel. The colon is scanned in distal direction, starting from the coecum to the rectum.
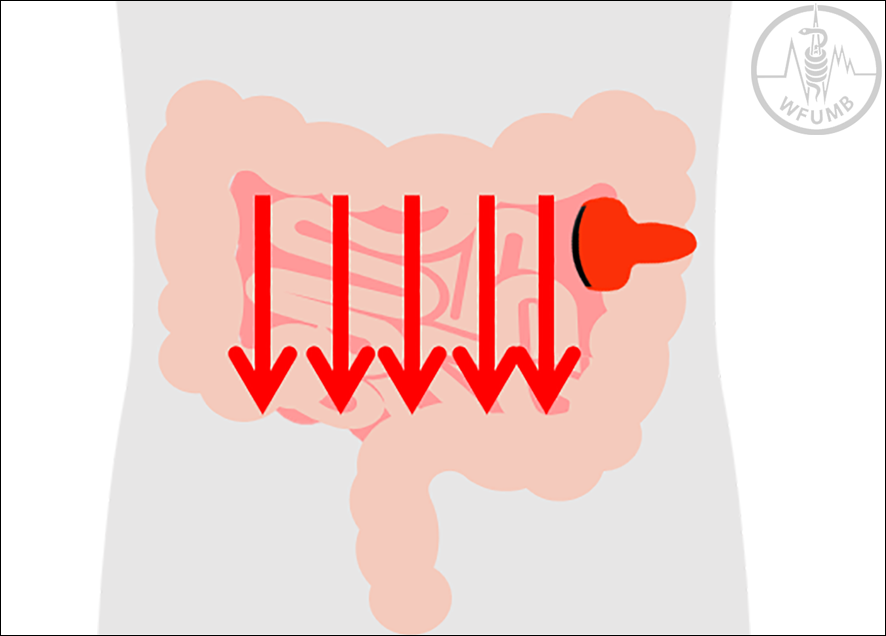
Fig 12.5a
Examination technique of the small bowel. The small bowel is scanned systematically by parallel overlapping scanning lanes (mowing the lawn) in vertical directions
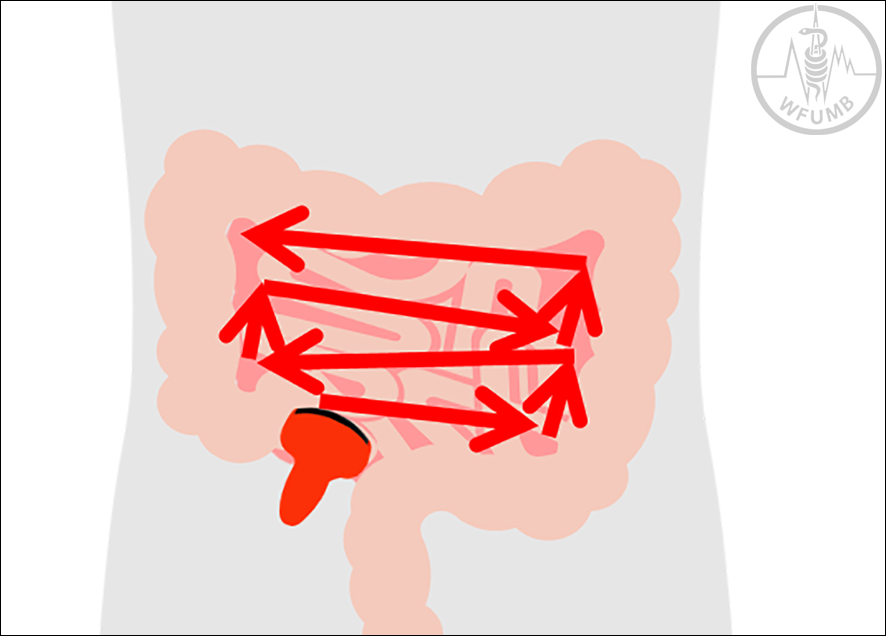
Fig 12.5b
Examination technique of the small bowel. The small bowel is scanned systematically by parallel overlapping scanning lanes (mowing the lawn) in horizontal directions
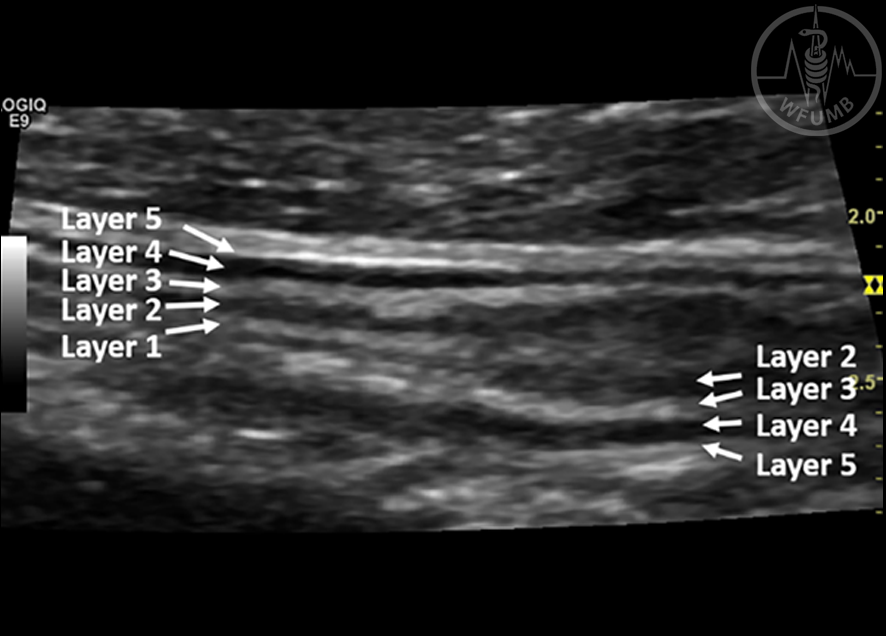
Fig 12.6
Five ultrasonographic wall layers corresponding to histological layers is depicted while the interpretation of the different layers is presented in the table below. The wall layers are numbered from the luminal side in this figure
Fig 12.7
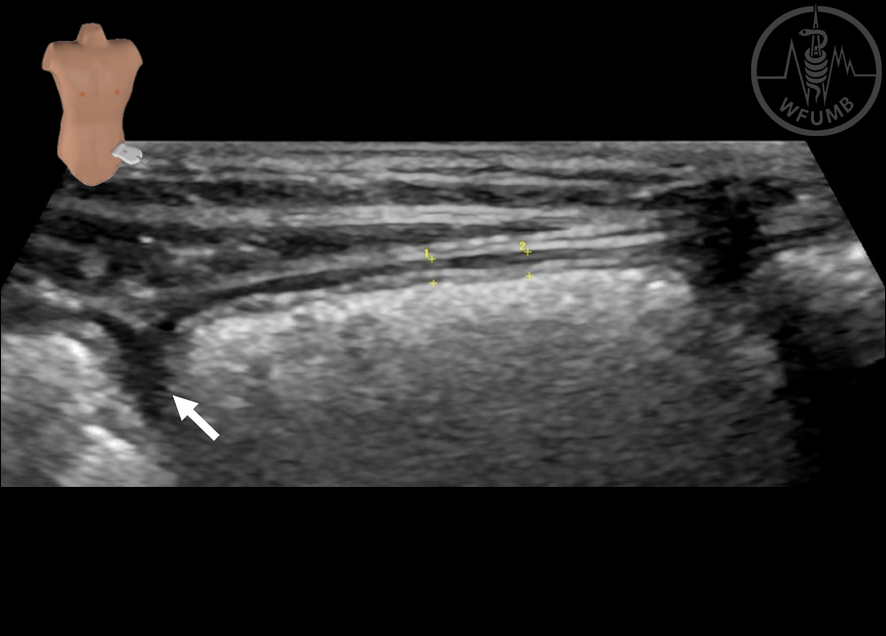
Measurement of bowel wall thickness (BWT) in a healthy colon. The BWT is measured from the start of the proper muscle to the end of the mucosal layer (between the yellow callipers). The measurements should be performed perpendicular to the anterior wall in longitudinal section. To avoid overestimation, the sonographer should omit measuring tangentially, in mucosal folds or in colonic haustrations (arrow)
Fig 12.8a
Healthy jejunal loops imaged in longitudinal section. Circular folds (arrow) are identified more frequently in the jejunal loops
Fig 12.8b
Healthy ileal loops imaged in longitudinal section. The luminal content has a fluid-like, greyish appearance (asterisk). The wall thickness (between yellow calipers) is usually less than 2 mm
Fig 12.9
The ileocecal valve (arrows) is identified as a short segment with increased wall thickness at the transition between the terminal ileum and the colon. Ileal (asterisk) and colonic (cross) segments are identified proximally and distally to the valve, respectively
Fig 12.10
A healthy colon imaged in longitudinal section. Haustration (arrows) is an important sonoanatomical characteristic and is depicted as a colonic protrusion. The faecal content (asterisk) is hyperechogenic as bowel gas is wrapped in the solid material. The wall thickness (between the yellow callipers) is usually less than 2 mm in distended colonic segments
Fig 12.11
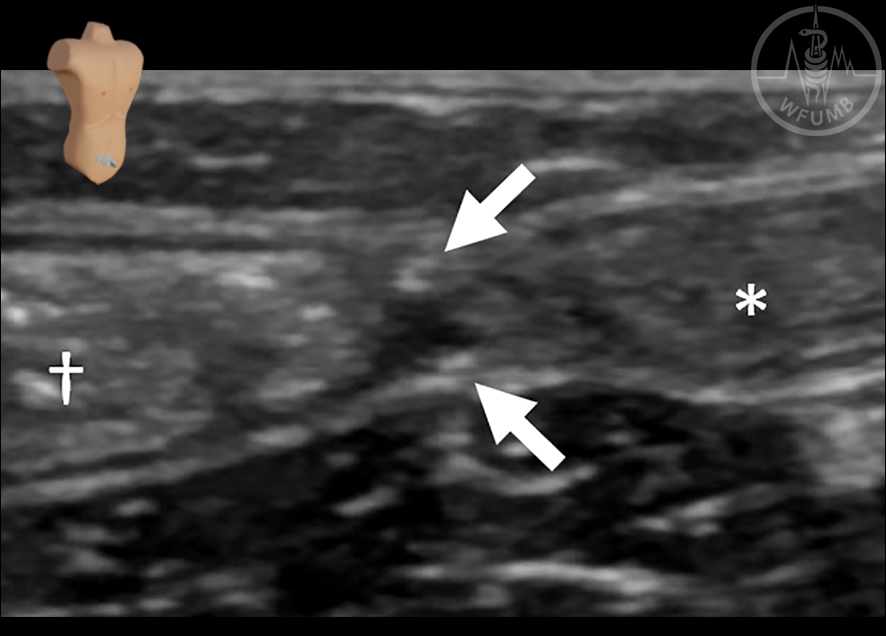
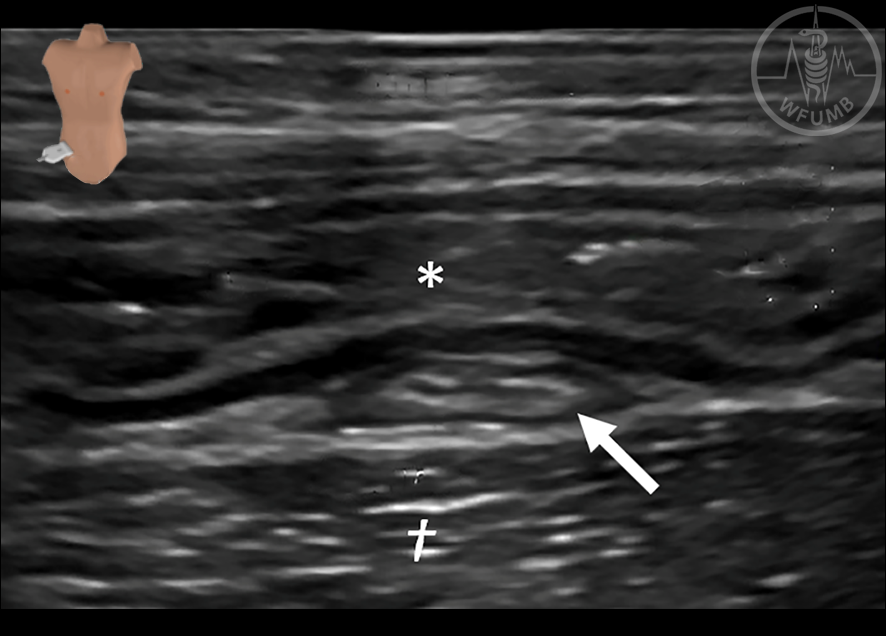
The sigmoid colon is located in the left fossa, positioned between the abdominal wall (asterisk) and the iliopsoas muscle (cross). The bowel segment collapses after
defecation, enabling the identification of both the anterior and posterior bowel walls (arrows)
Fig 12.12
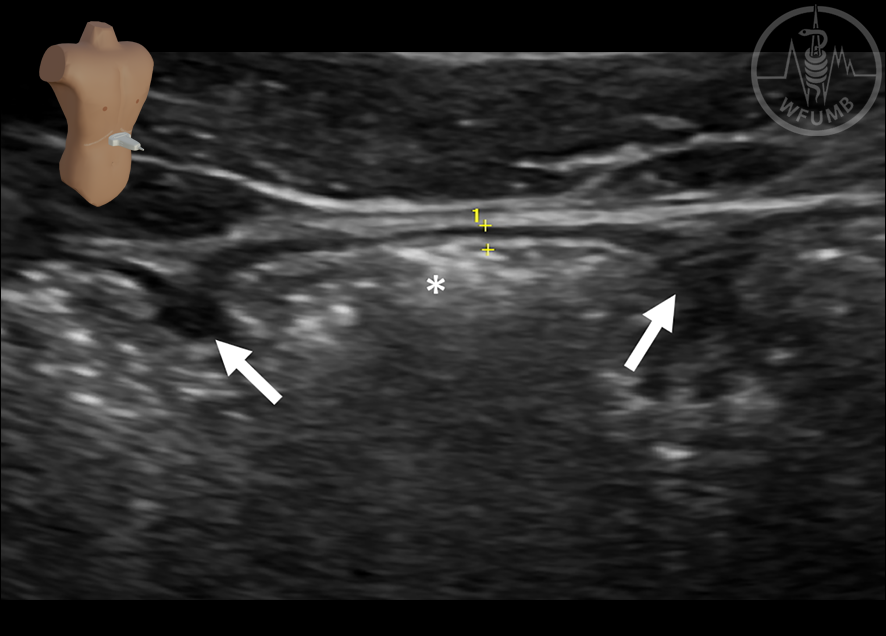
The appendix (arrow) is found between the terminal ileum (asterisk) and the iliopsoas muscle (cross). A healthy appendix should be easy to compress as illustrated in this figure