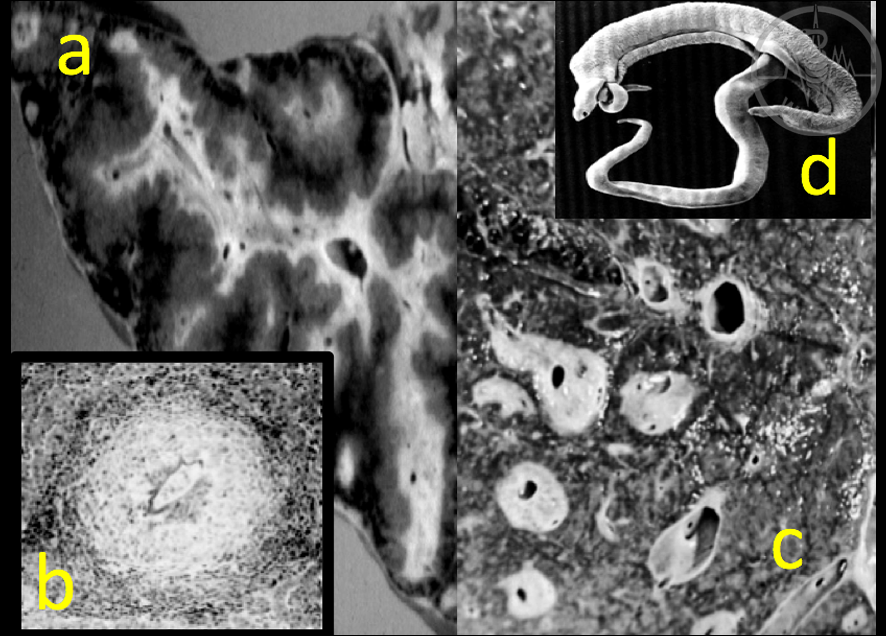
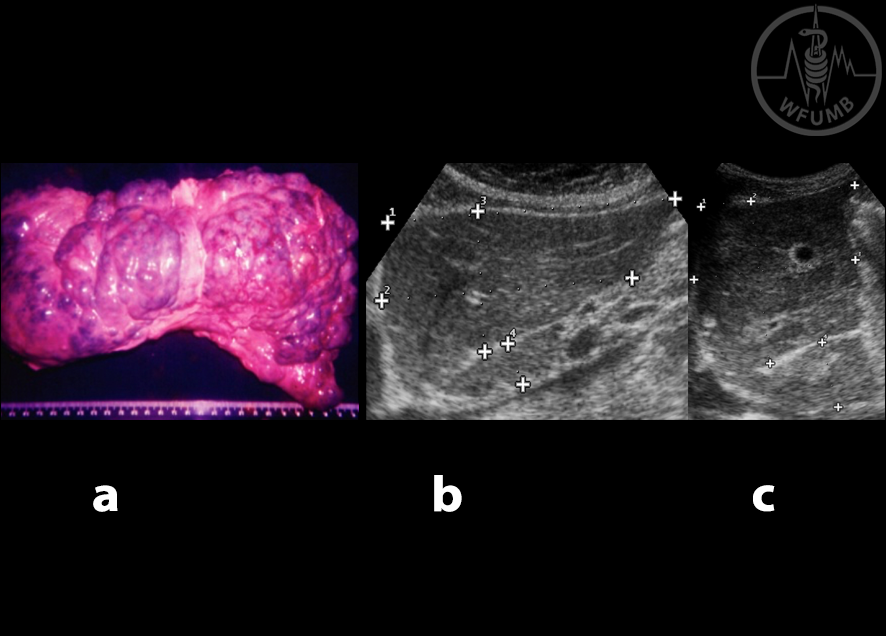
Fig 23.1
SCH periportal fibrosis is determined by the intense granulomatous immune reaction of the host to the highly antigenic eggs of the parasite. a. Hepatic linear fibrosis of the portal tracts (resected specimen).
b. Intense fibrosis around SCH eggs. c. Liver fibrosis (transversely resected specimen). d. SCH parasite
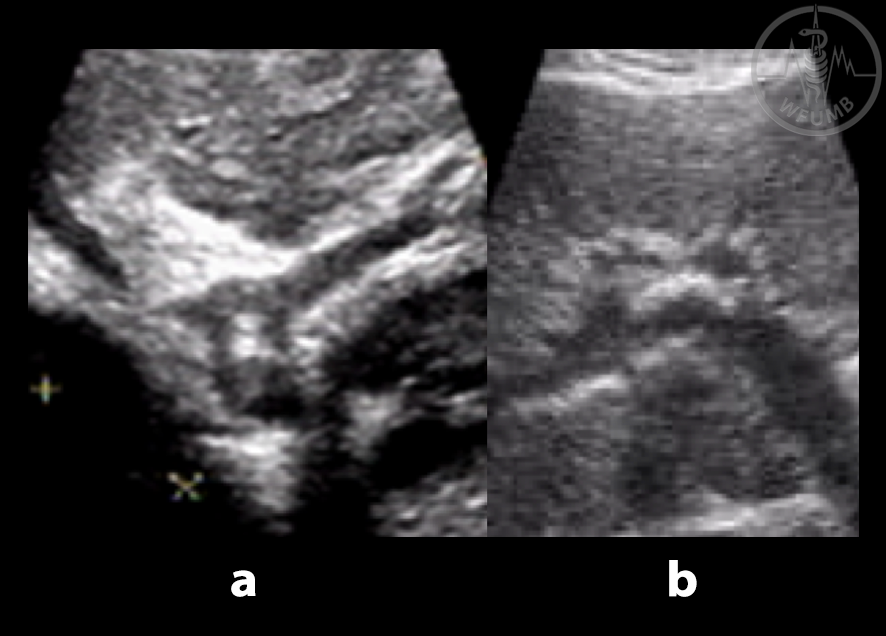
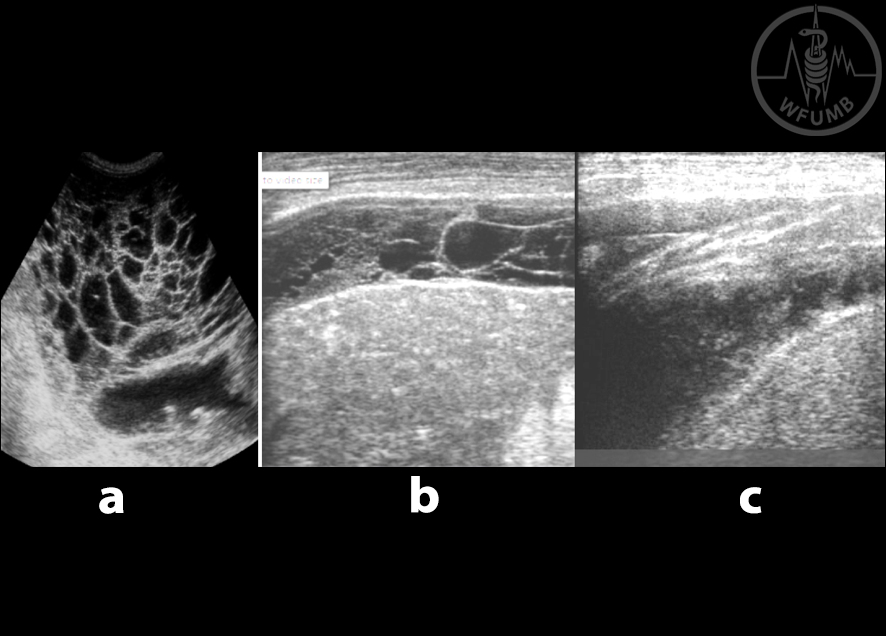
Fig 23.2
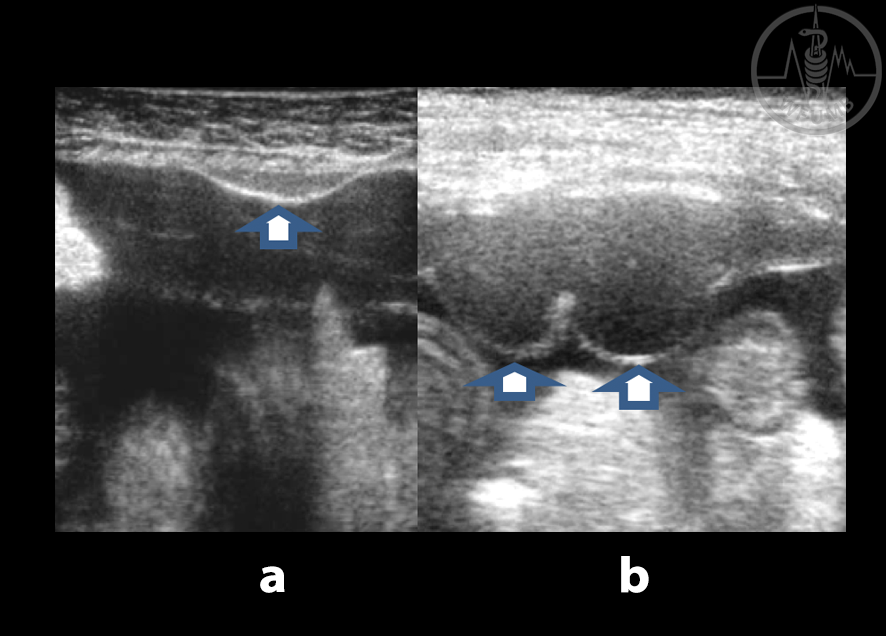
Extensive keloid wall thickening is diagnostic of SCH periportal fibrosis on US scan. a. Longitudinal view of portal tracts.
b. Transverse view. c. Main PV (fibrosis thickness 1.3cm)
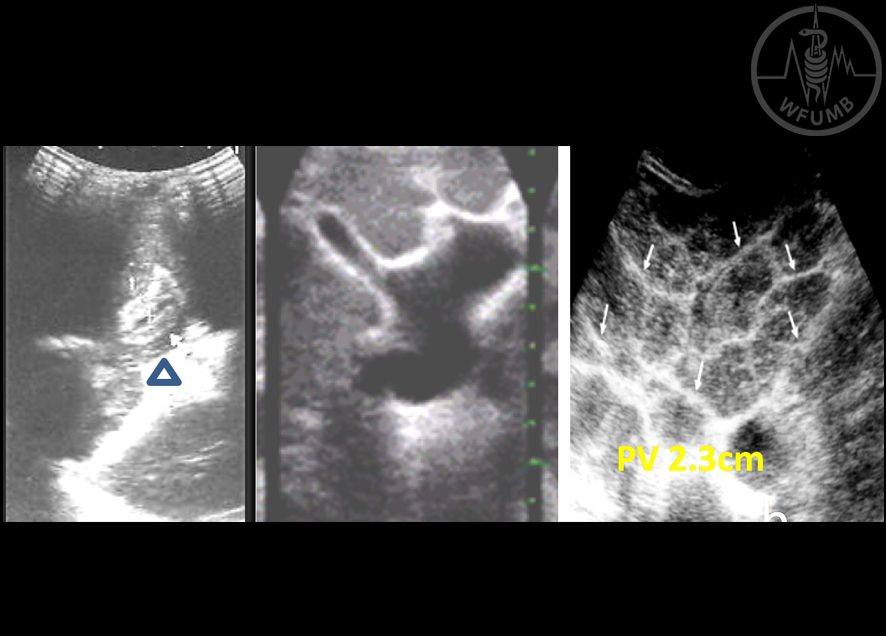
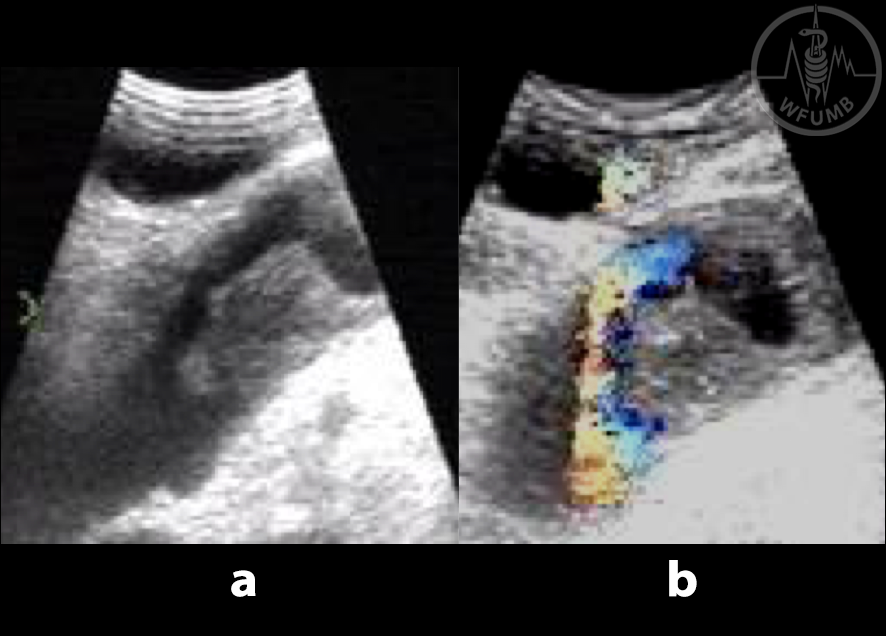
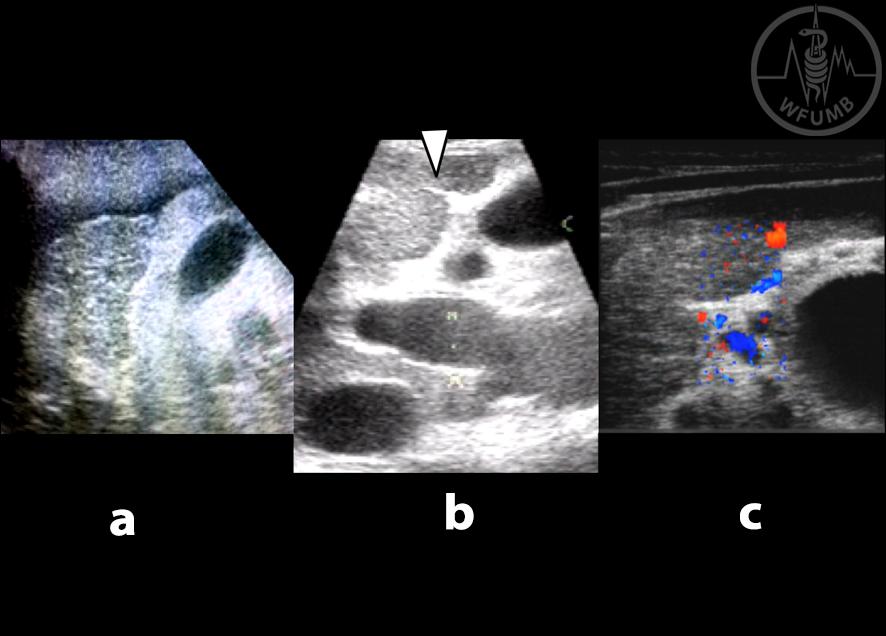
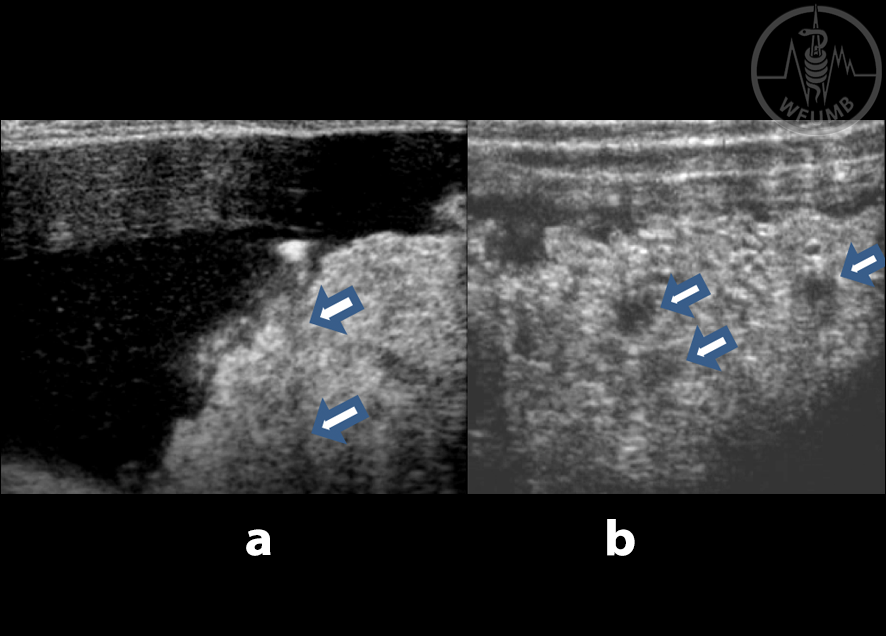
Fig 23.3
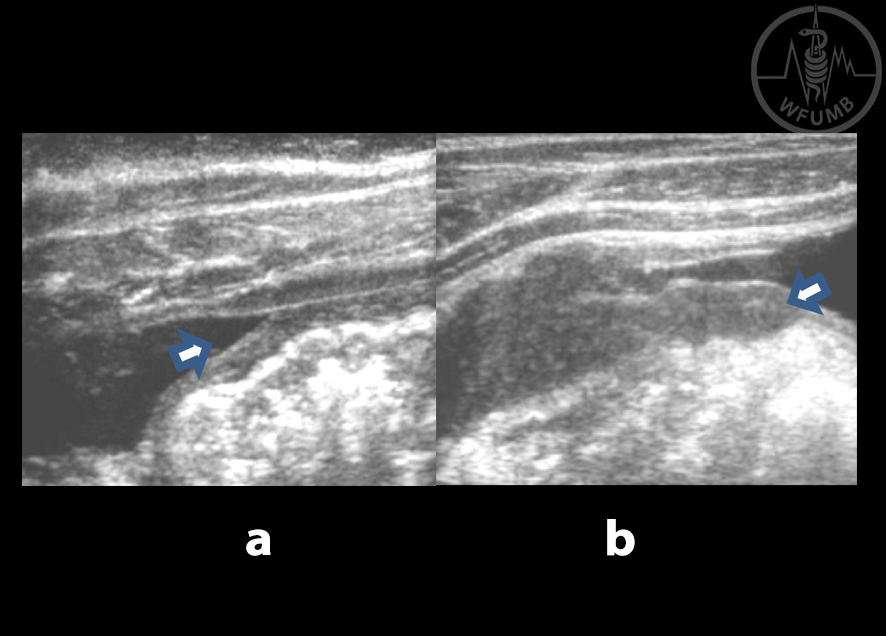
US images of periportal fibrosis showing. a. Regular fibrosis. b. Luminal dilatation of the left and main PV.
c. SCH Japonicum
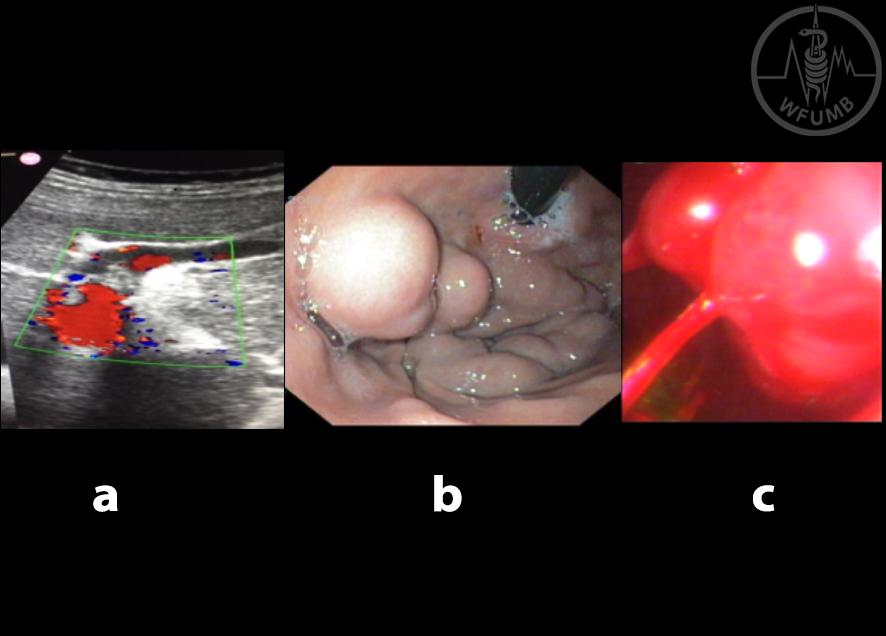
Fig 23.4
Photos and images describing severity of SCH portal hypertension.
a. Recanalized para umbilical vein on US.
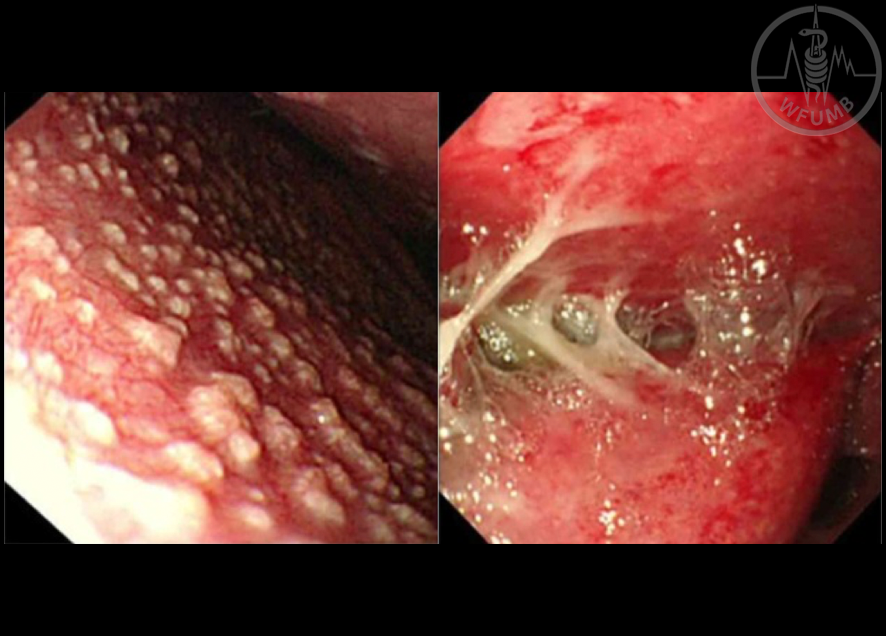
b. Gastric varices (endoscopy).
c. Bleeding esophageal varix (endoscopy)
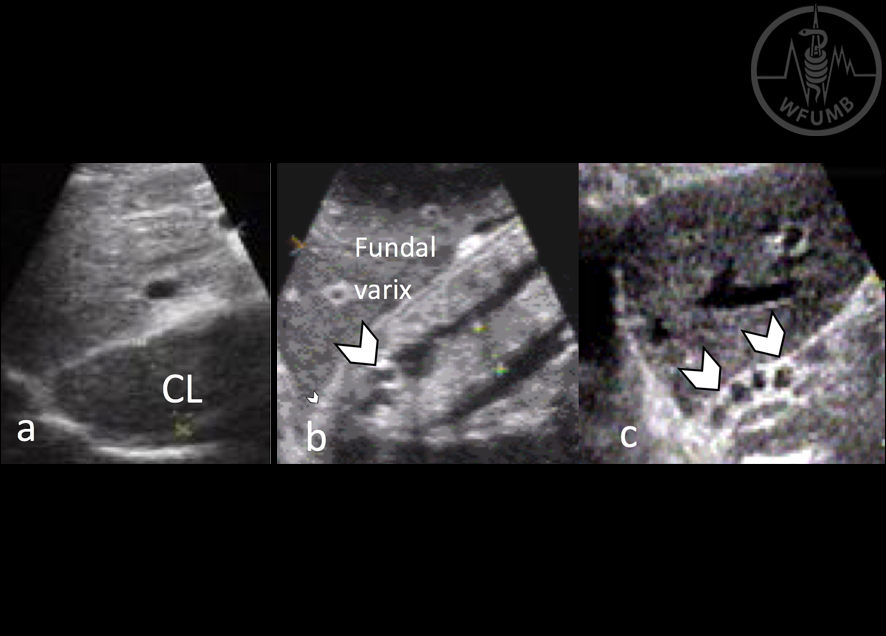
Fig 23.5
Ultrasonographic evidence of PH in SCH periportal fibrosis. a. Enlarged caudate lobe. b. Gastropathy and gastric varix. c. Junctional esophageal varices
Fig 23.6
a. Autopsy specimen of a SCH liver displaying the paradoxical enlargement of the left lobe and shrinkage of the right lobe. b. US scan of a normal left lobe contrasted to that of a SCH left lobe in c.
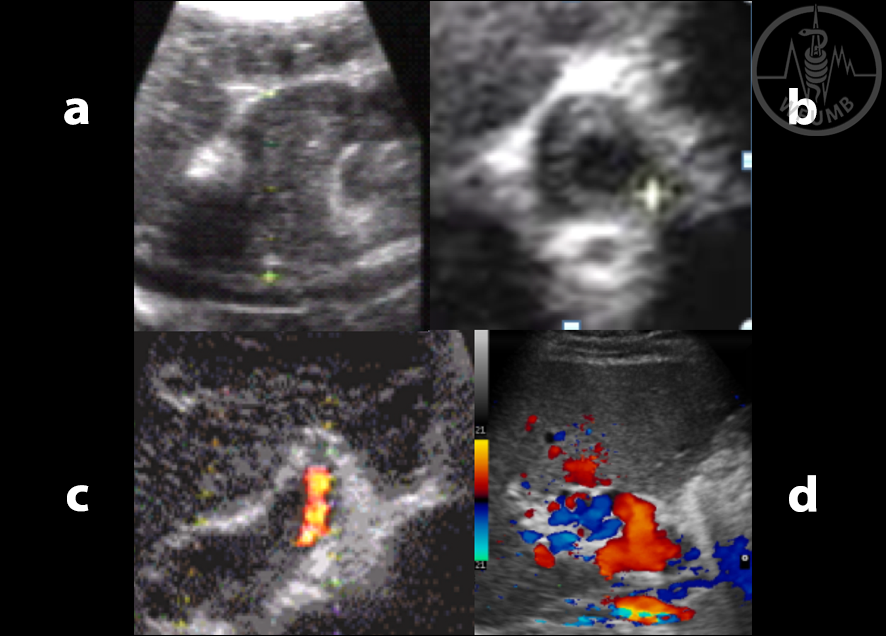
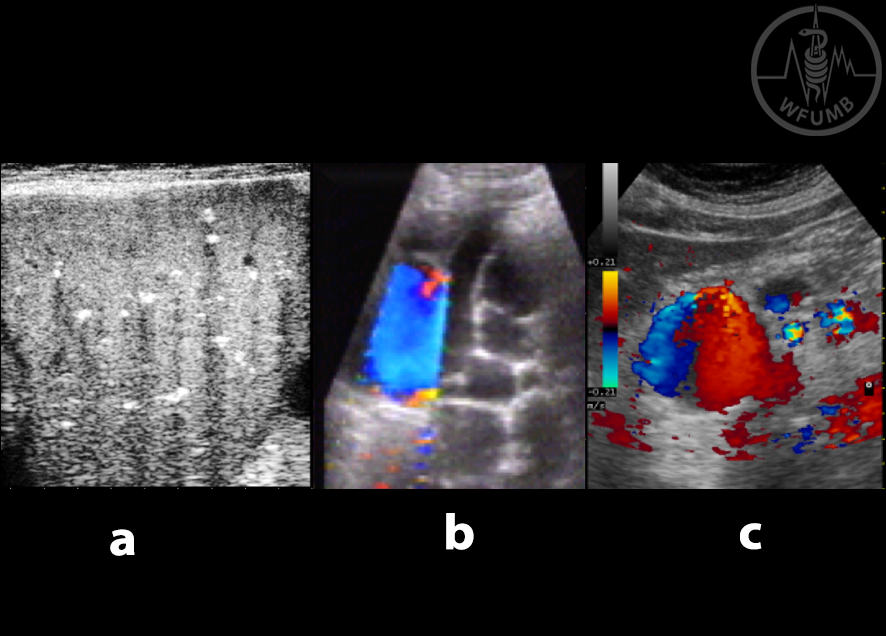
Fig 23.7
a. and b. Examples of PV thrombosis. c. secondary left portal branch thrombosis. d. PV cavernoma
Fig 23.8
a. and b. PV calcifications in SCH due to presence of eggs or dead worms
Fig 23.9
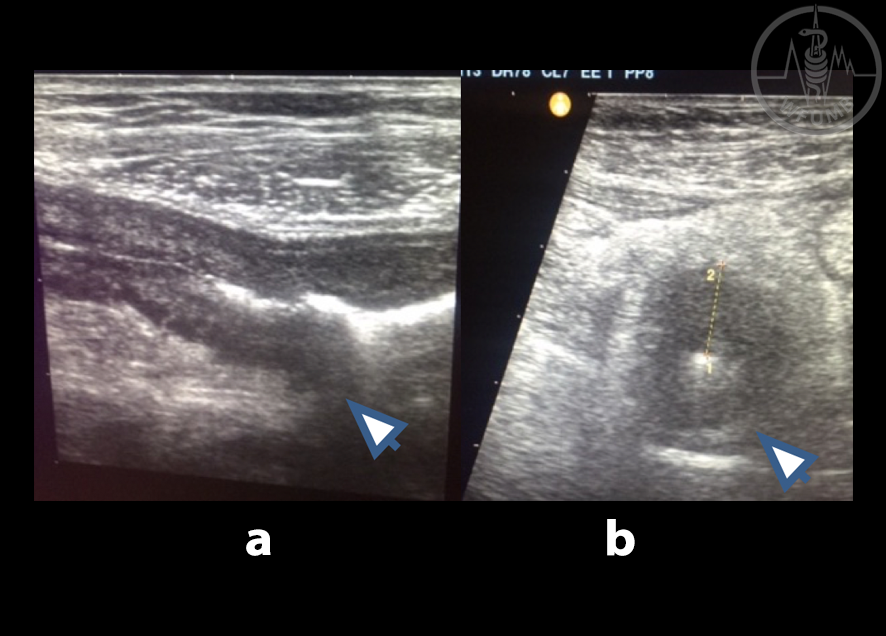
SV can be extremely wide, up to 2.5cm. Thrombosis and calcifications are not uncommon. a. and b.
Examples of splenic vein thrombosis
Fig 23.10
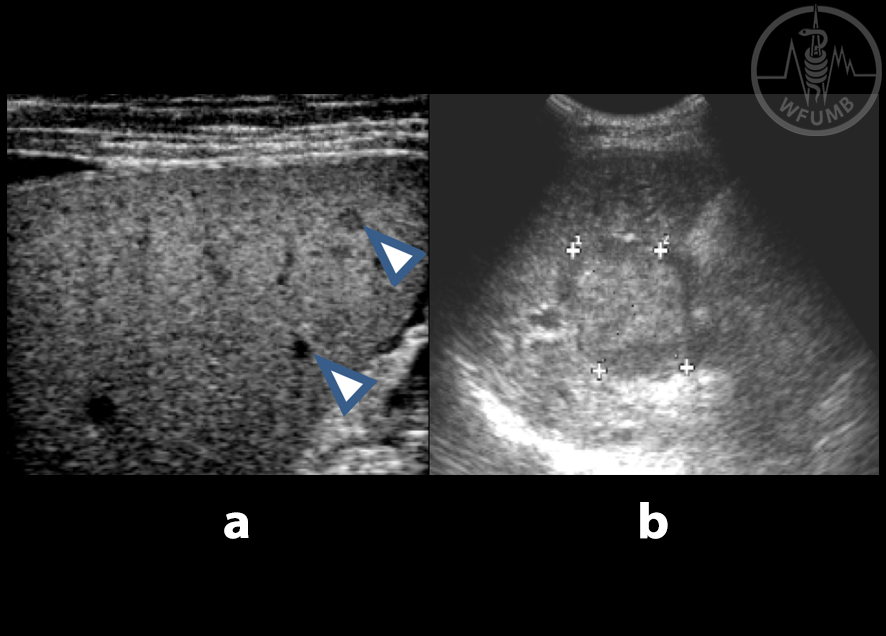
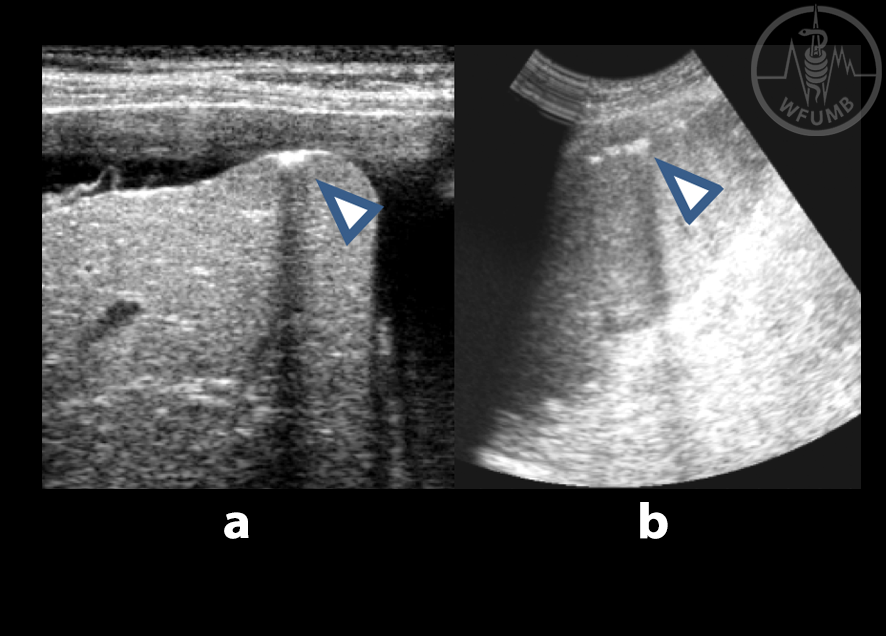
a. Marked thickening of the fibrotic wall of the GB (2.3cm). b. Spiky fibrous projections penetrate the adjacent liver parenchyma (arrow). c. Collaterals in GB wall especially prominent with PV thrombosis
Fig 23.11
a. Spleen with calcification shadows. b. Splenic hilar collaterals - wide and rich, if absent an alternative site eg, epigastrium, peripancreatic or pelvic locations should be explored. c. Epigastric collaterals (diameter 3.4cm) in a patient with absent splenic hilar collaterals
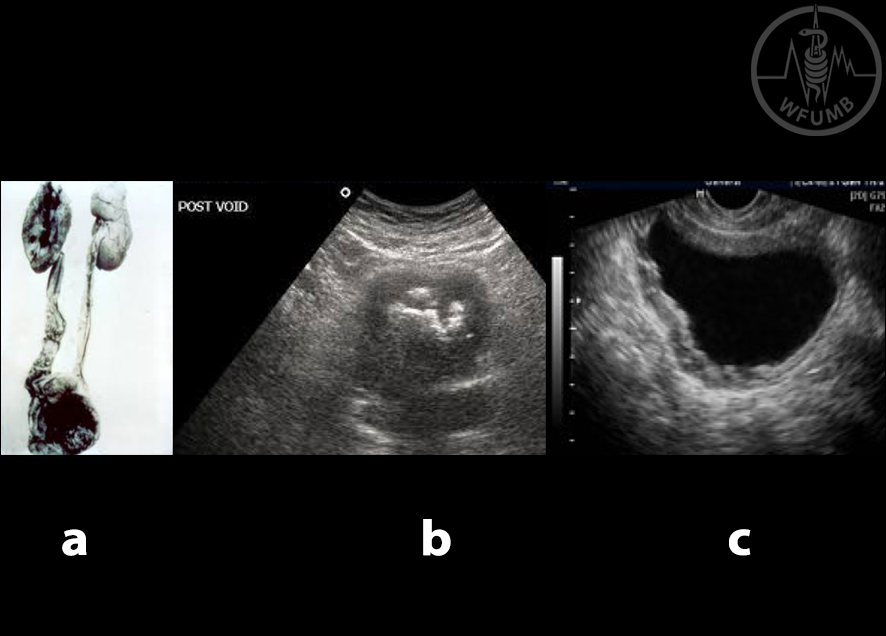
Fig 23.12
a. Vesico ureteric orifice fibrosis resulting in hydroureteronephrosis (anatomic piece). b. US scan of bladder showing calcification and c. wall thickening in
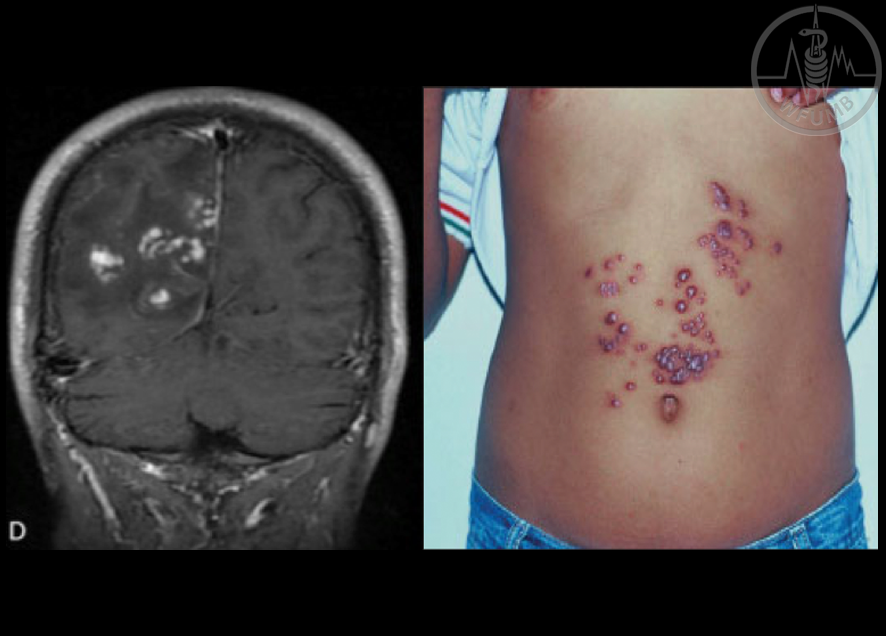
Fig.23.13
Example of ectopic SCH affecting brain and skin
Fig 23.14
Laparoscopic view of TB tubercles in a. peritoneum, b. peritoneal adhesions
Fig 23.15
Abdominal lymphadenitis, common finding in abdominal TB. a. porta hepatis LN (arrow).
b. Epigastric LN, calcification shown is a credited sign to TB (arrow). c. Peripancreatic LN (arrow)
Fig 23.16
a. and b. Nodular peritoneal thickening in abdominal TB
Fig 23.17
Parietal and visceral peritoneal thickening in abdominal TB. a. Global peritoneal thickening (arrow). b. Segmental peritoneal thickening (arrow)
Fig 23.18
Terminal ileum in intestinal TB. a. longitudinal view.
b. Cross section view (wall thickness 1.3cm)
Fig 23.19
Omentum growth. a. With calcification spots (arrows pointing to the shadow)
b. With infiltrations (arrows)
Fig 23.20
TB peritoneal adhesions visible as linear hyperechoic structures floating in the ascitic fluid, when extensive appearing like compact honeycomb. a. Abdominal adhesions. b. Adhesions overlying liver. c. Overlying the spleen
Fig 23.21
Abdominal collections in 2 separate patients (a. and b.) Occasionally punctate calcifications are seen within
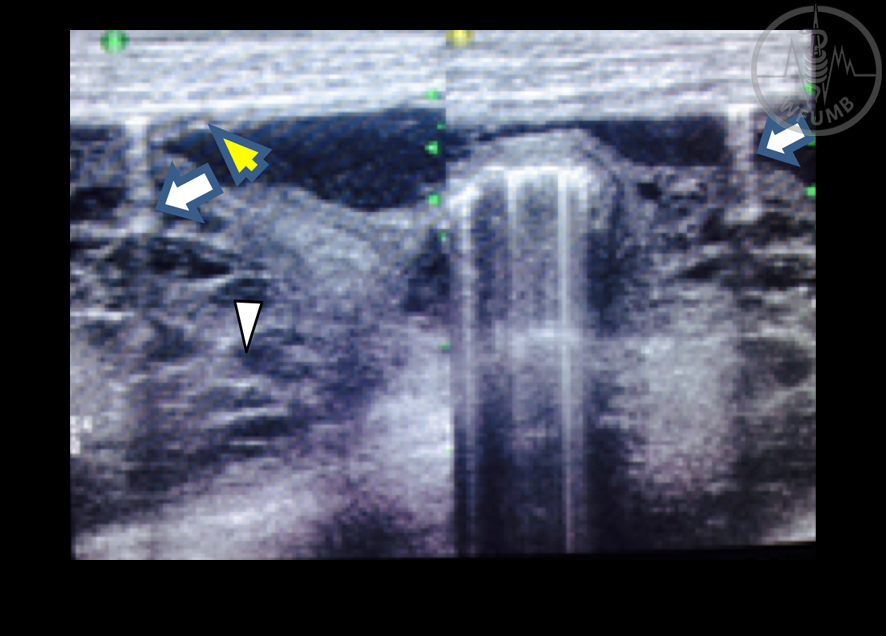
Fig 23.22
Perforated bowel in a complicated case of abdominal TB. Note the free peritoneum gas (white arrow), the adhesions (arrow head) and the minor peritoneal thickening (yellow arrow)
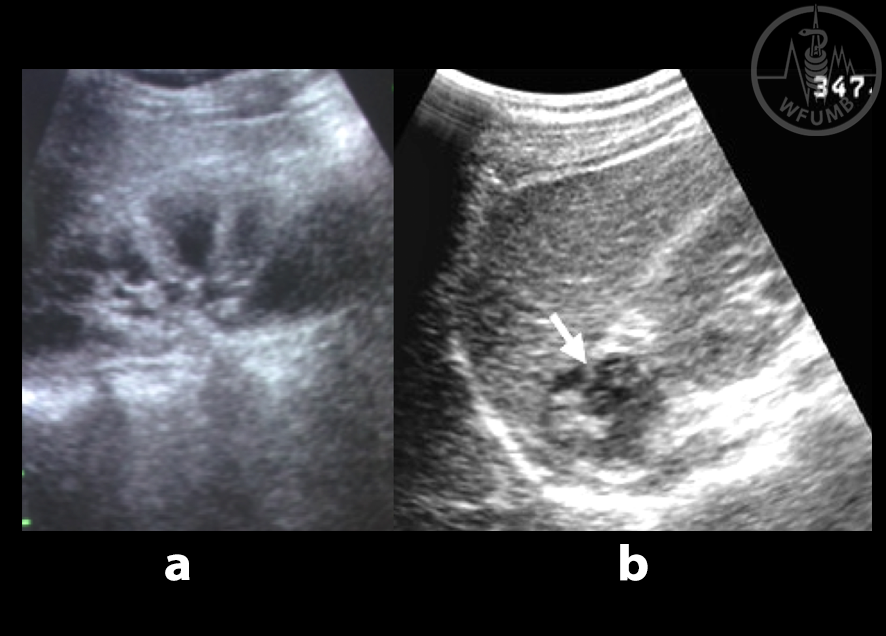
Fig 23.23
Hepatic TB. a. Hepatic calcification inside a hypoechoic focal lesion. b. Hepatic tubercloma.
c. Punctate calcification of liver in hepatic TB
Fig 23.24
a. Spleen TB infiltration
b. Spleen tubercloma
Fig 23.25
Surface calcification (arrows). a. Liver b. Spleen
Fig 23.26
55 years-old lady with chylous ascites secondary to abdominal TB. Note the white content of the bag
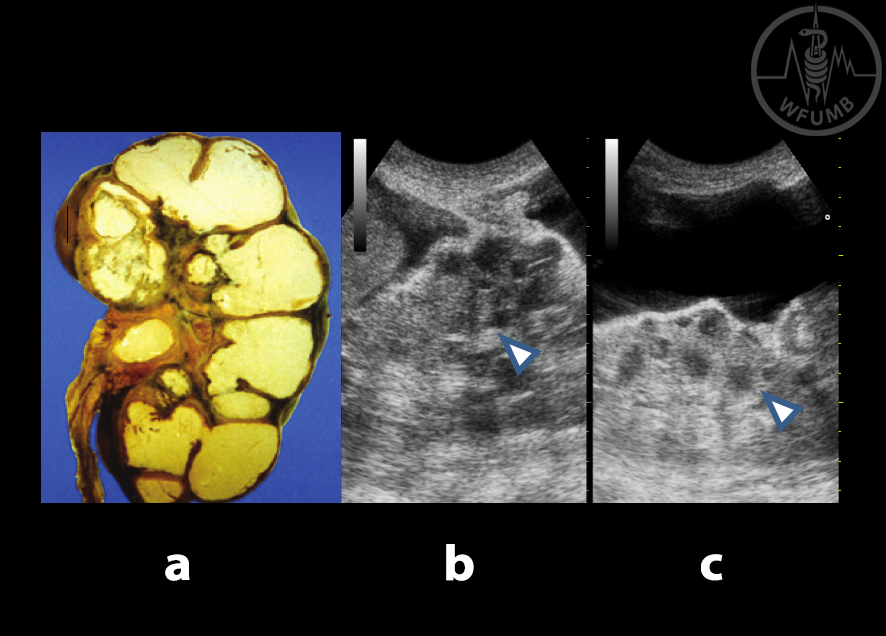
Fig 23.27
Renal TB. a. Nephrectomy specimen; renal tissue replaced by caseous material. b. and c. US view showing severe distortion of renal architecture in renal TB (poor differentiation of the parenchyma vs. basinet) in a middle age male with sterile pyuria and infertility
Fig 23.28
a. Tuberculous renal atrophy (note the calcifications) b. Adrenal enlargement with calcification (arrow)
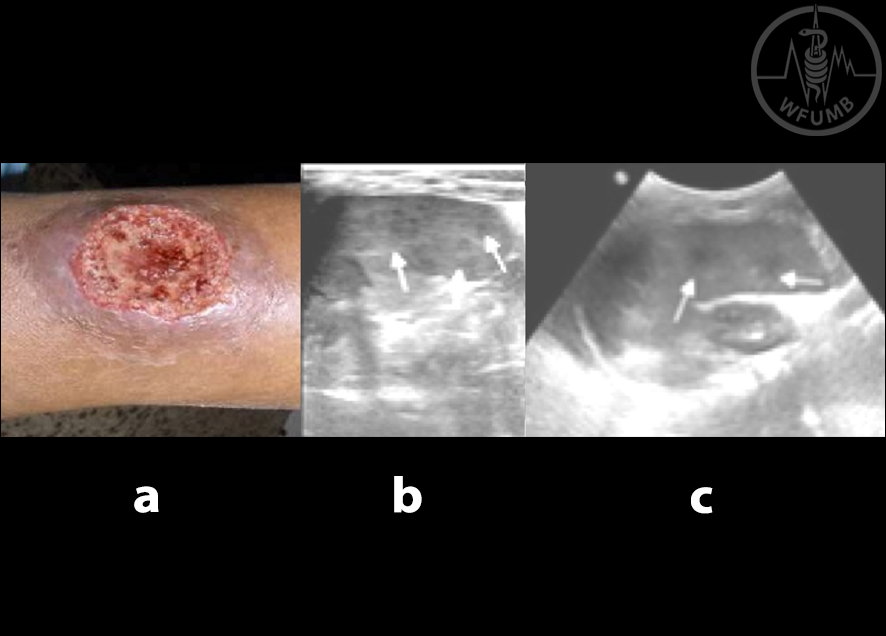
Fig 23.29
a. Cutaneous Leishmaniasis. b. and c. Spleen sonography of Leishmania patients showing splenomegaly with multiple small iso-hypoechoic nodules (arrows)
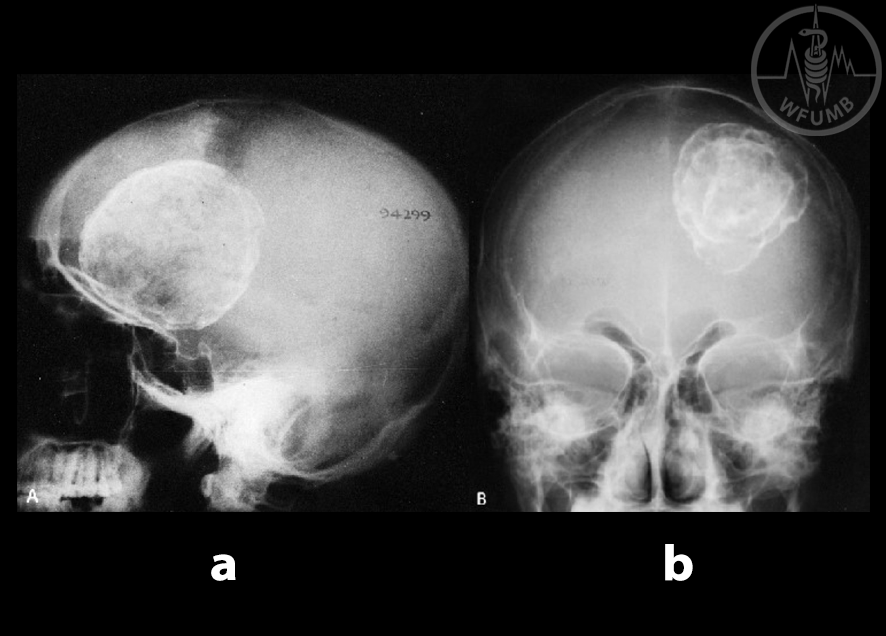
Fig 23.30
Plain radiographs, profile a. and frontal b. skull views: Calcified HC in the left fronto-parietal region of the brain in a 15-year-old boy
Fig 23.31
HA Gharbi doing US abdominal screening in Tunis children’s hospital testing a portable machine CGR 100D
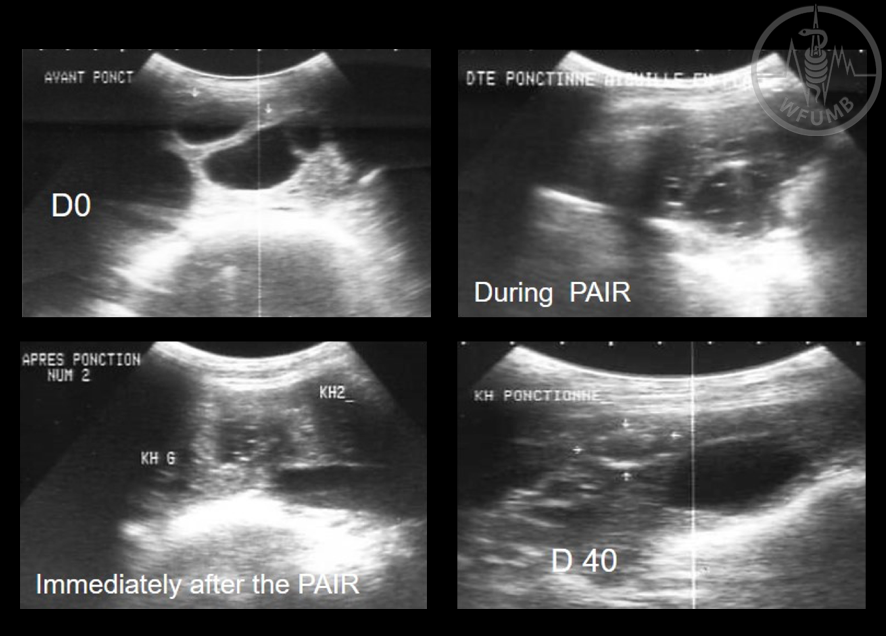
Fig 23.32
PAIR technique (dipeptide methyl) for treatment of hydatid cysts used in sheep (F Ben Chehida)