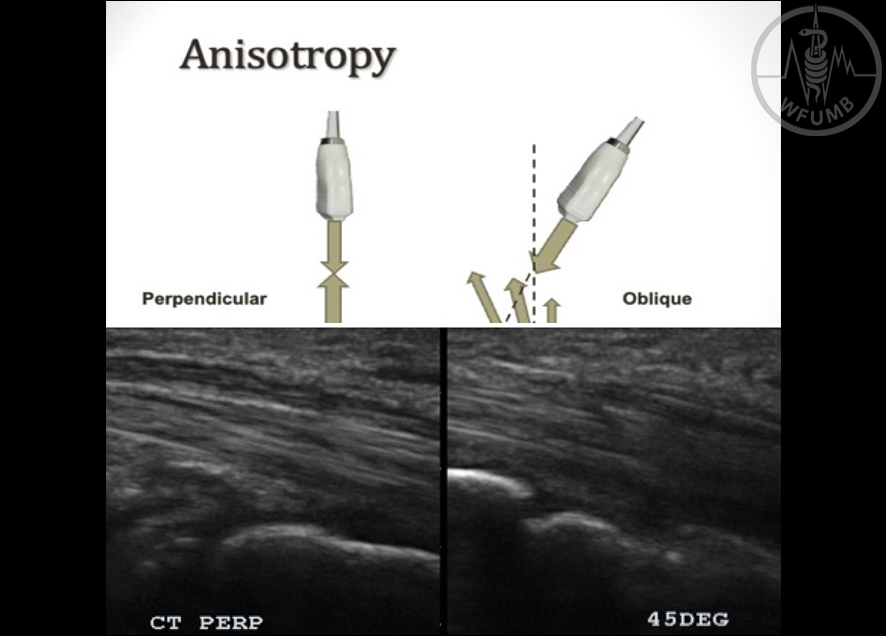
Fig 24.1
Altering the angle of reflectance between perpendicular and closer to parallel and then back to perpendicular again the tendon go from light to dark, and then back to light as the angle of the transducer is shifted
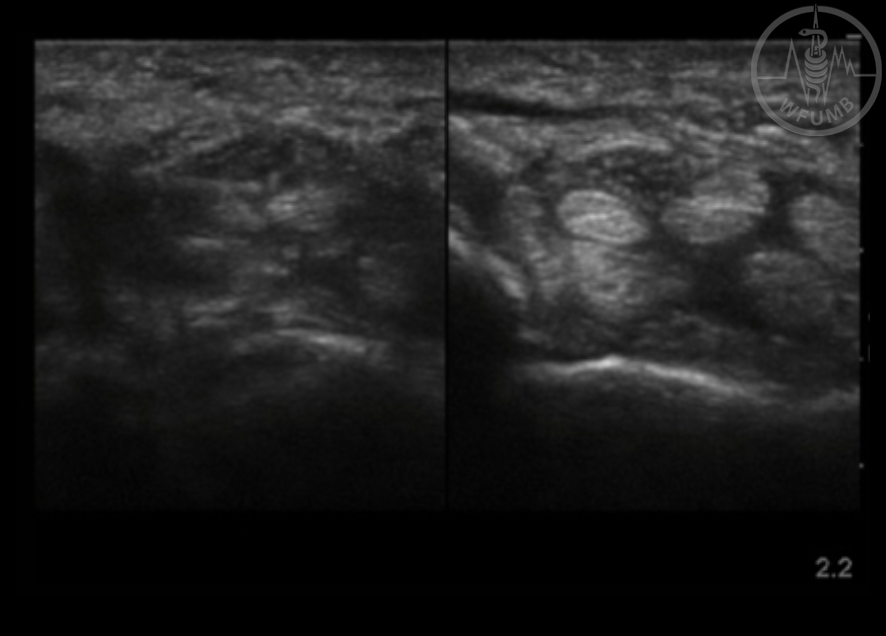
Fig 24.2
Image of carpal tunnel perpendicular and at 45 degrees showing degree of anisotropy in tendons vs median nerve at both angles
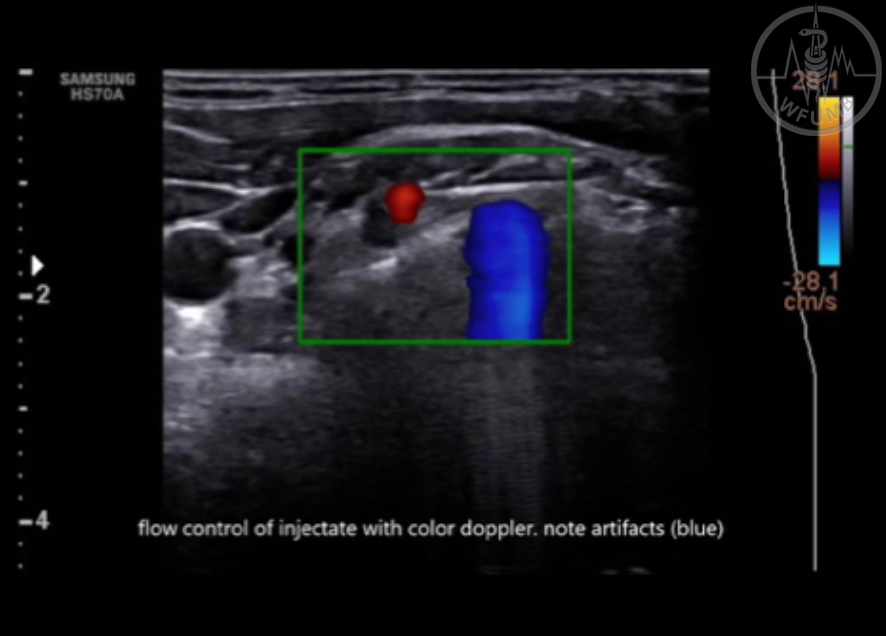
Fig 24.3
Ultrasound guided injection of C6 cervical root
(Courtesy Dr. Marco La Grua)
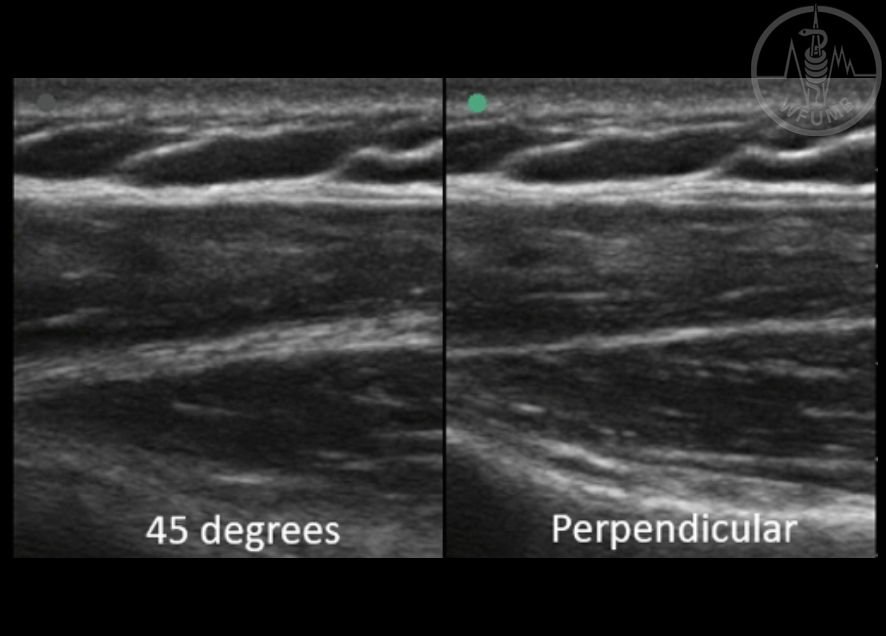
Fig 24.4
Image of fascial plane between anterior and medial deltoid at perpendicular vs 45-degree angle
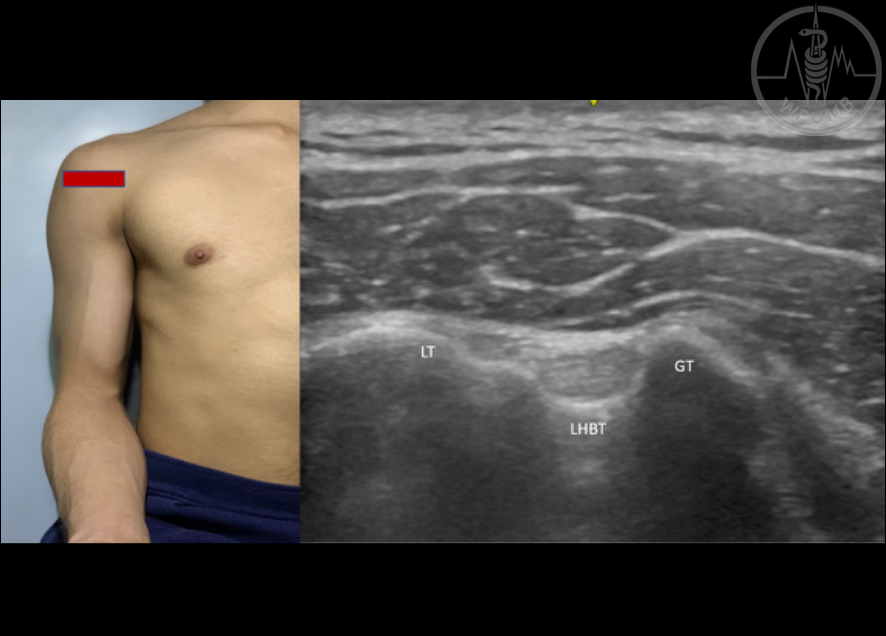
Fig 24.5a
Shoulder scanning protocol - long head of the biceps tendon in short axis (SAX). Position - Patient’s shoulder is adducted, elbow flexed 90degrees, forearm and hand supinated (LT: Lesser Tubercle, LHBT: Long head of the biceps tendon, GT: Greater tubercle)
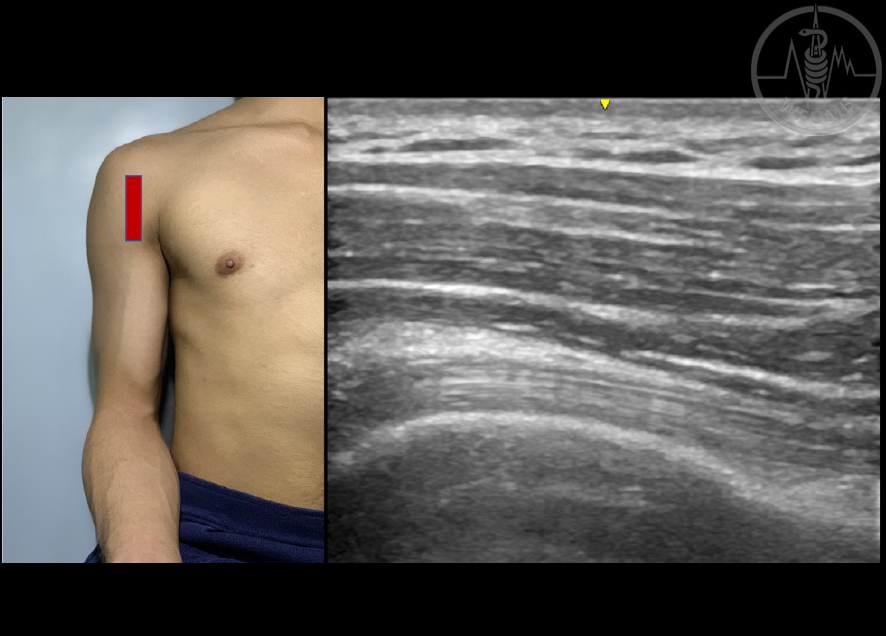
Fig 24.5b
Shoulder scanning protocol - long head of the biceps tendon in long axis (LAX). Position - Shoulder adducted, elbow flexed 90 degrees, forearm and hand supinated. Hyperechoic, fibrillar pattern of the long head of the biceps tendon is visualized in long axis.
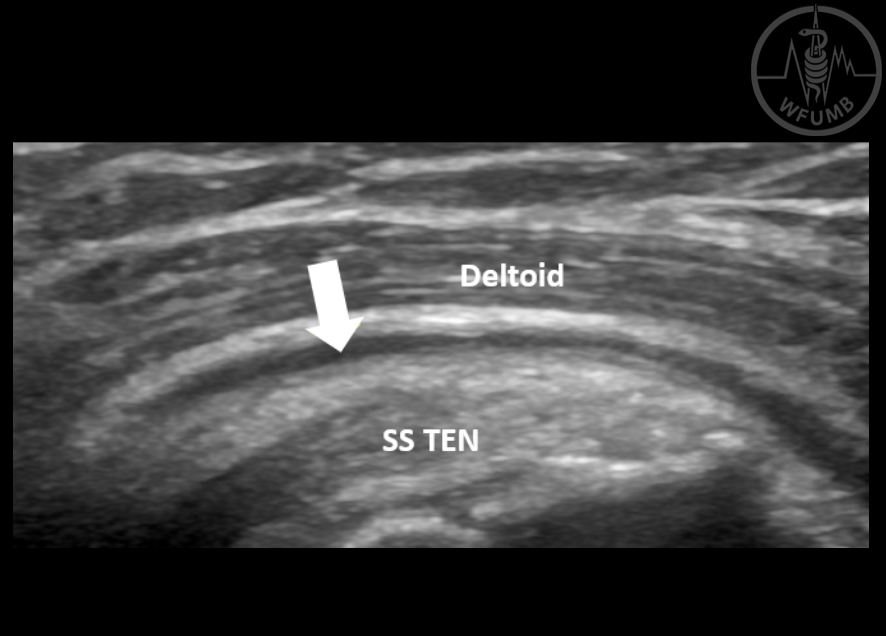
Fig 24.6
Calcific tendinopathy of supraspinatus tendon (shoulder). Hyperechoic calcification at the articular portion of the tendon (arrow)
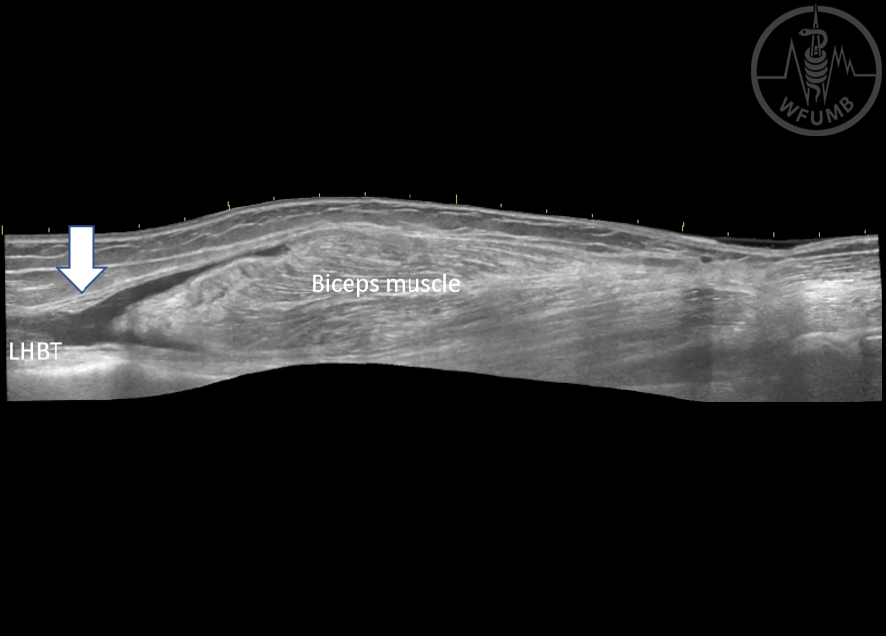
Fig 24.7
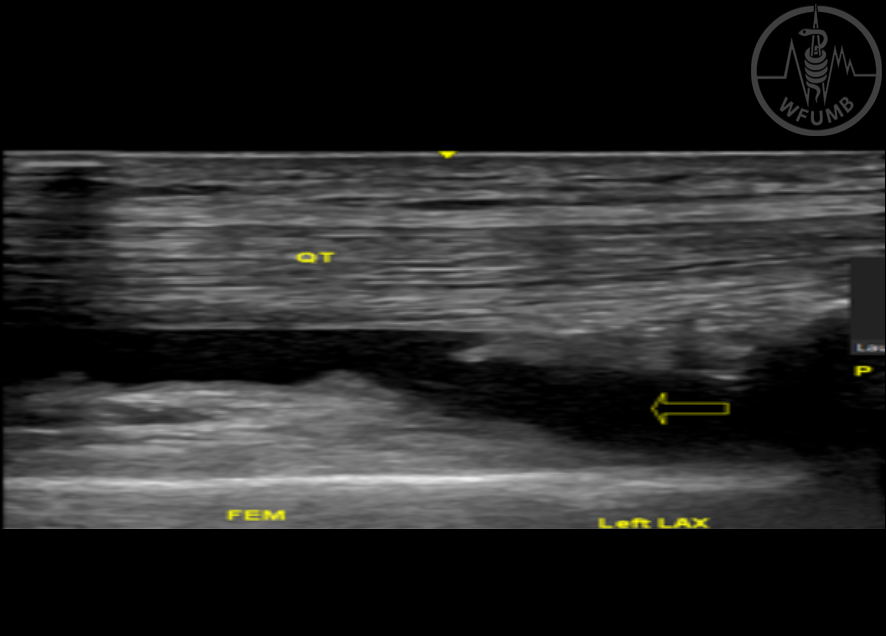
Long head of the biceps tendon rupture (shoulder). Anechoic discontinuation of the long head of the biceps tendon at the myotendinous junction (white arrow) (LHBT: Long head of the biceps tendon)
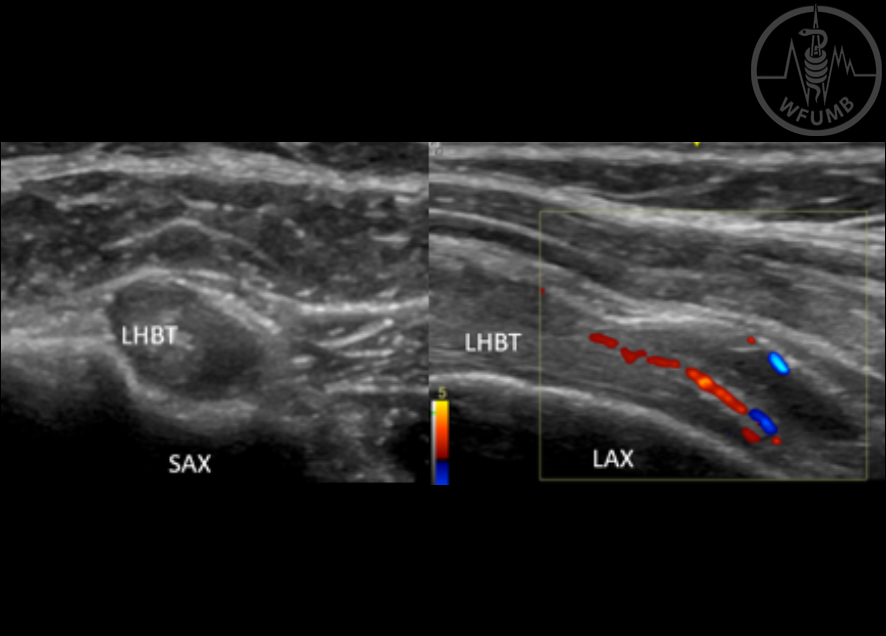
Fig 24.8
Long head of the biceps tenosynovitis (shoulder) Presence of anechoic peritendinous effusion surrounding the long head of the biceps tendon (LHBT) visualized on short axis (SAX) long axis (LAX). There is also increase in hyperemia on the color Doppler study in LAX
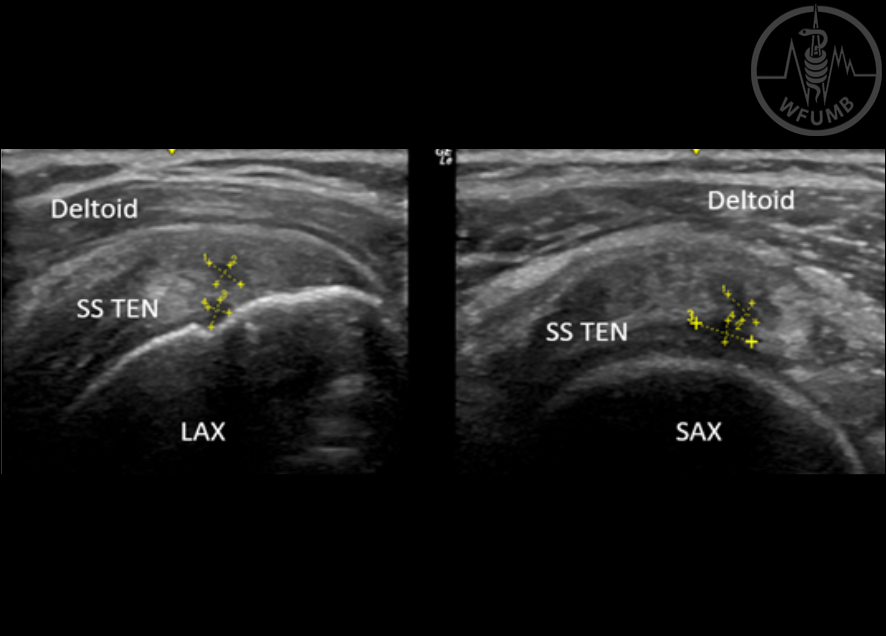
Fig 24.9
Supraspinatus multifocal tear (shoulder). Anechoic area with partial fiber disruption at the intrasubstance and at the articular part visualized in both long axis (LAX) and short axis (SAX) views (SSTEN: Supraspinatus tendon)
Fig 24.10 Subdeltoid bursitis (shoulder). Anechoic dilatation of the subdeltoid bursa (SS TEN: Supraspinatus tendon)
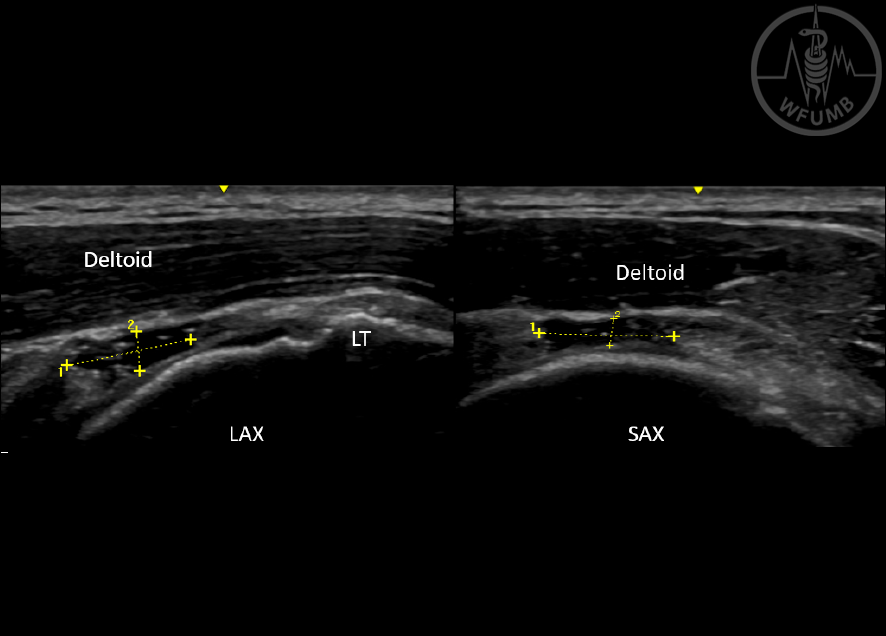
Fig 24.11
Full thickness tear of supraspinatus tendon (shoulder). Anechoic fiber disruption from the articular extending to the bursal part. Tear is visualized on long axis (LAX) and short axis (SAX) views
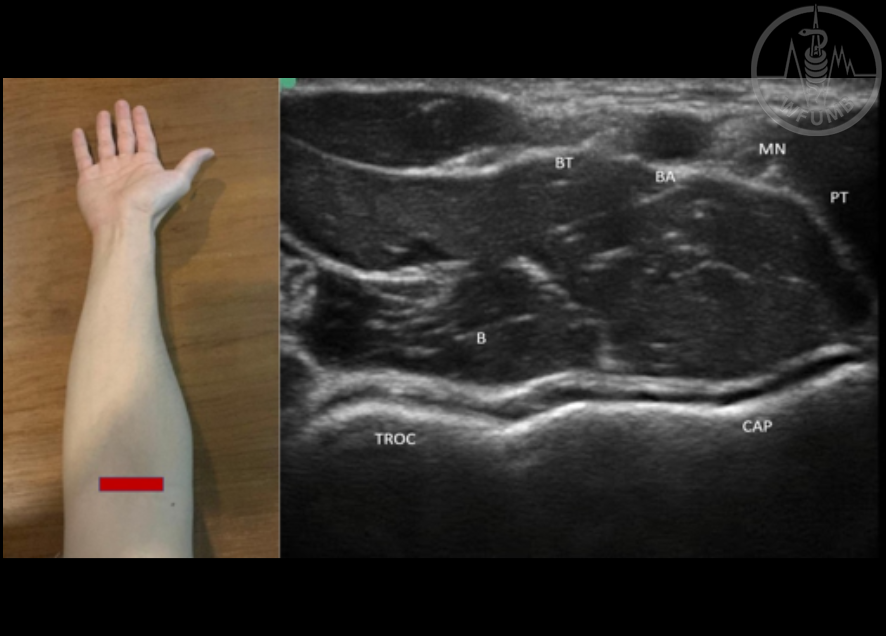
Fig 24.12a
Elbow scanning protocol - anterior elbow short axis (SAX). Position: Patient is seated or supine with the elbow extended, forearm and hand supinated. (BT: Distal biceps tendon, a hyperechoic superficial structure; BA: Brachial artery, an anechoic pulsating structure; MN: Median Nerve, a hypoechoic honeycomb structure; PT: Pronator teres muscle; B: Brachialis; TROC: Trochlear surface; CAP: Capitellum).
Fig 24.12b
Elbow scanning protocol - anterior elbow long axis (LAX). Position: Patient is seated or supine with the elbow extended, forearm and hand supinated. Arrows: Distal Bicep Tendon
Fig 24.13
Lateral epicondylitis (elbow). Hypoechoic thickening of the common extensor tendon at the insertion site into the lateral epicondyle
Fig 24.14
Olecranon bursitis (elbow). Anechoic dilatation of the olecranon bursa (TP: Triceps tendon)
Fig 24.15a
Wrist and hand scanning protocol - volar aspect. Carpal tunnel short axis (SAX). Position: Hand is supinated and placed on the examination tab (FCRT: Flexor carpi radialis tendon, S: Scaphoid bone, White arrow: Median Nerve (Honeycomb appearance), RA: Radial artery, P: pisiform).
Fig 24.15b
Wrist and hand scanning protocol - volar aspect. A1 pulley. Position: Probe is placed between the metacarpal and proximal phalanx (Arrow: A1 pulley, FDS: Flexor digitorum superficialis, FDP, Flexor digitorum profundus, MCP: metacarpal bone, PI: Proximal Phalanx)
Fig 24.16
De Quervain’s tenosynovitis (wrist). Anechoic peritendinous effusion (open arrow) surrounding the abductor pollicis longus tendon and extensor pollicis brevis tendon
Fig 24.17
Ganglion cyst (wrist). Anechoic mass superior to the scapholunate ligament
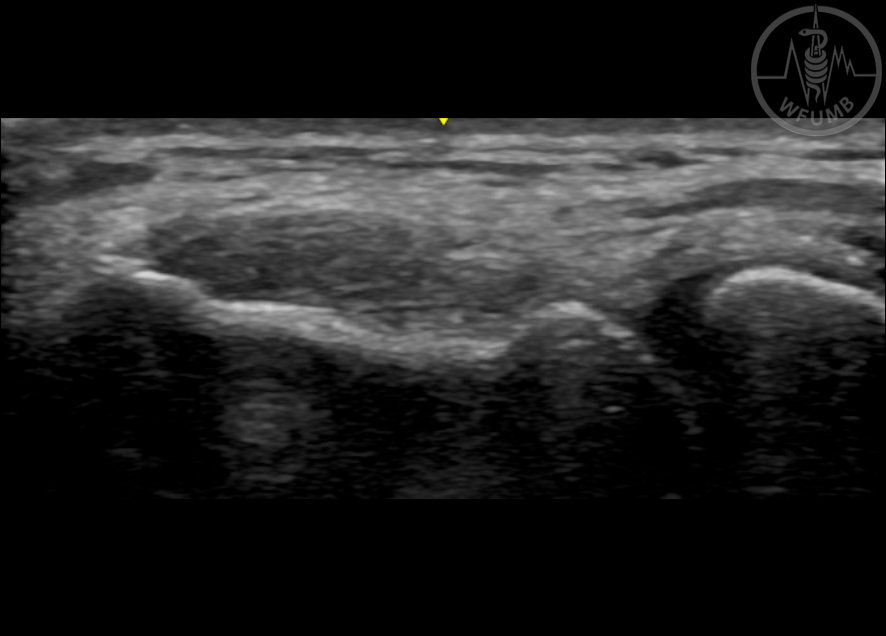
Fig 24.20
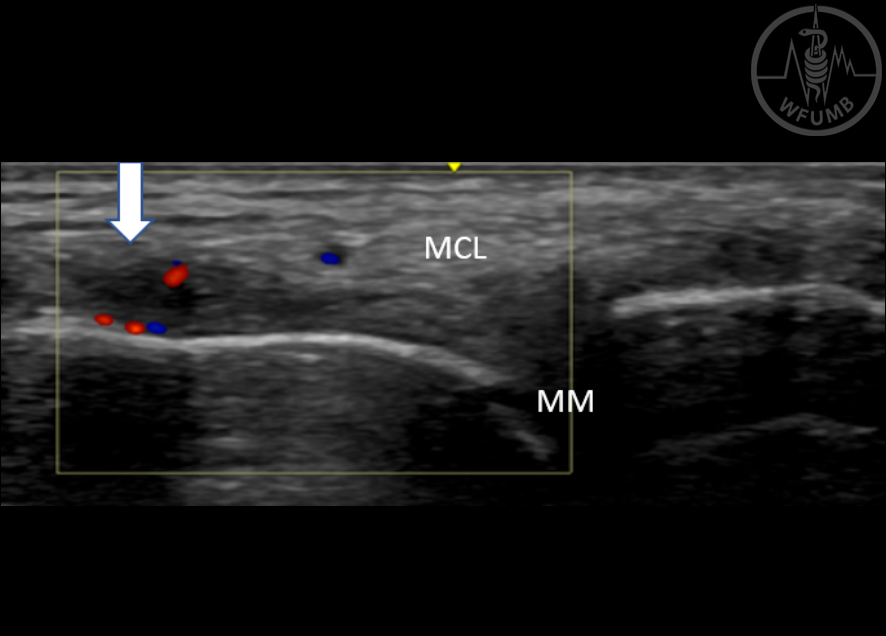
Medial collateral ligament (MCL) sprain (knee). Anechoic fiber disruption at the proximal part of the MCL (MCL: Media Collateral Ligament, MM: Medial Meniscus)
Fig 24.21
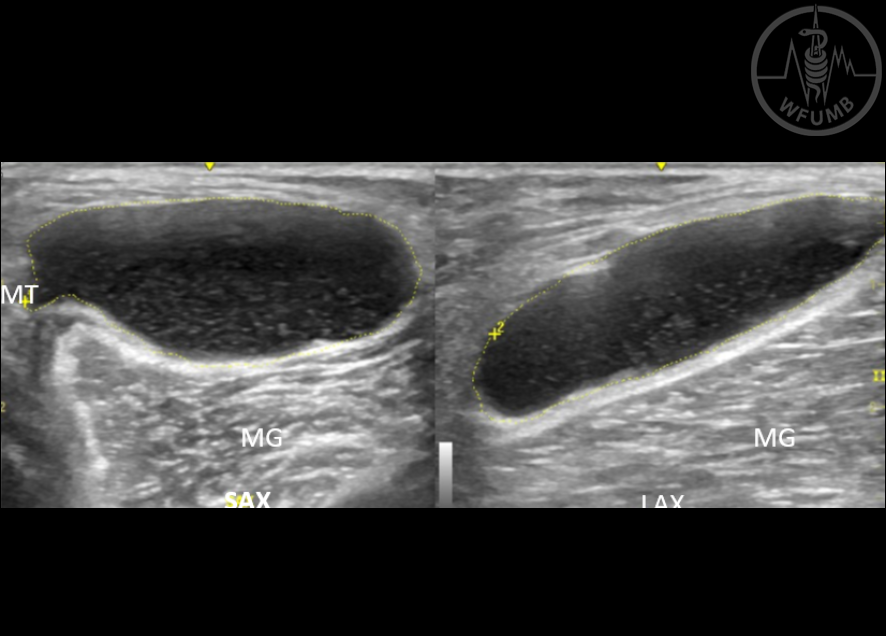
Baker’s cyst (knee). Anechoic cyst between the semimembranosus tendon (SMT) and the medial gastrocnemius muscle (MG)
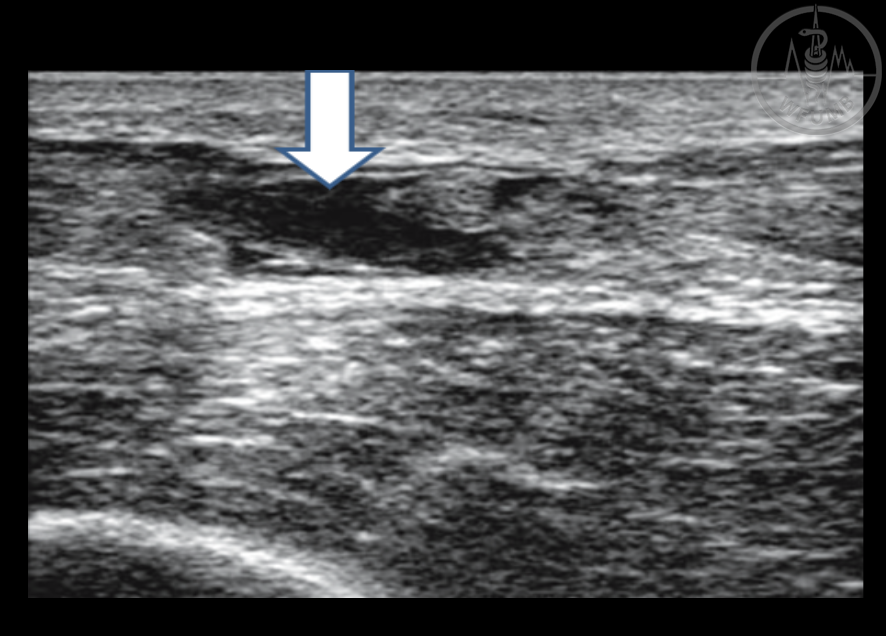
Fig 24.22
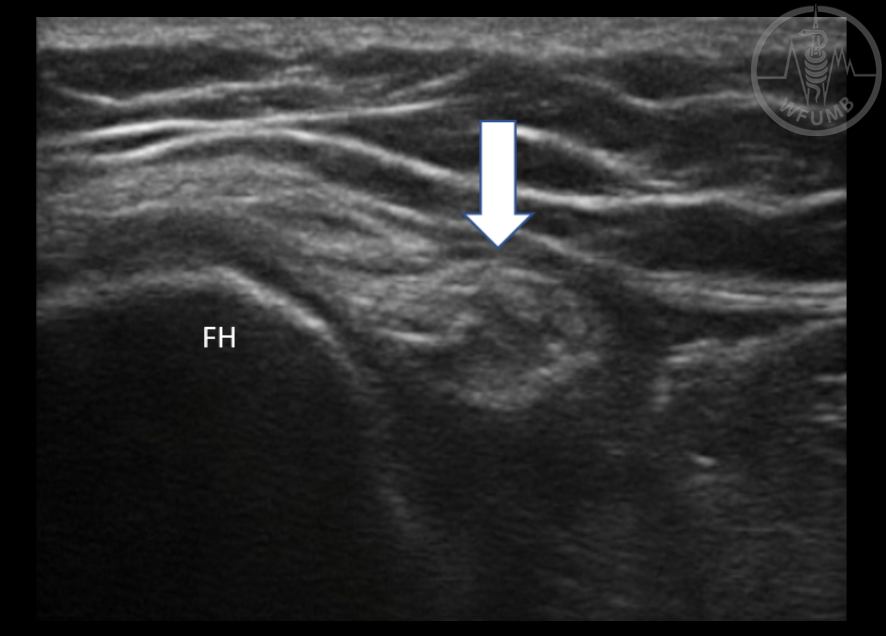
Common peroneal neuropathy (knee). Hypoechoic enlargement of the common peroneal nerve (White arrow) at the level of the fibular head (FH)
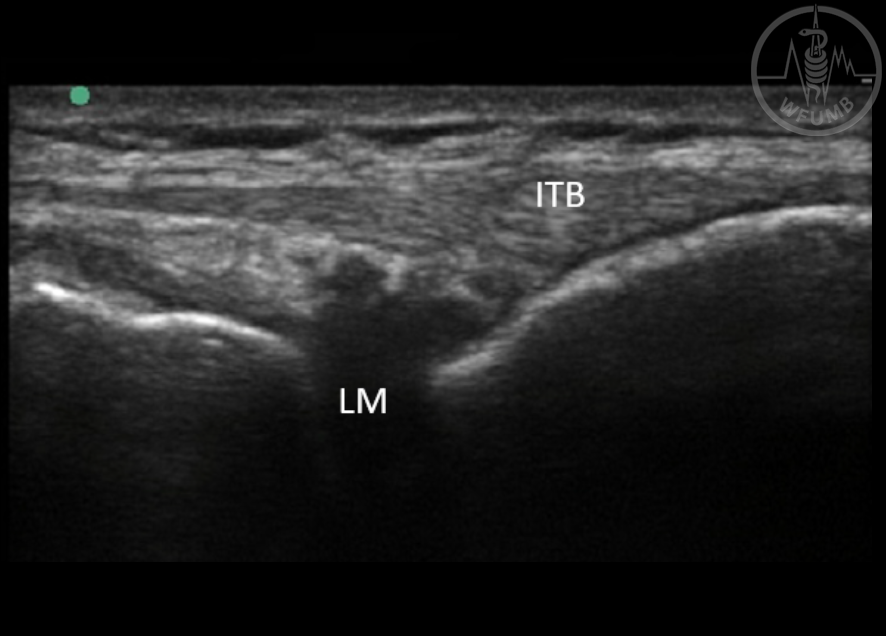
Fig 24.23
Lateral meniscus tear (knee). Anechoic disruption of the lateral meniscus (LM) (ITB: Iliotibial band)
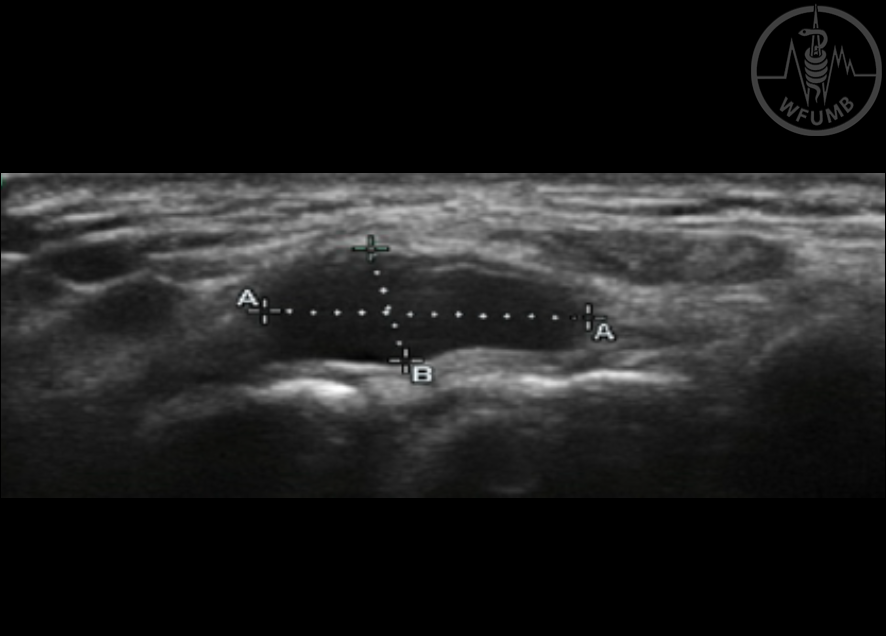
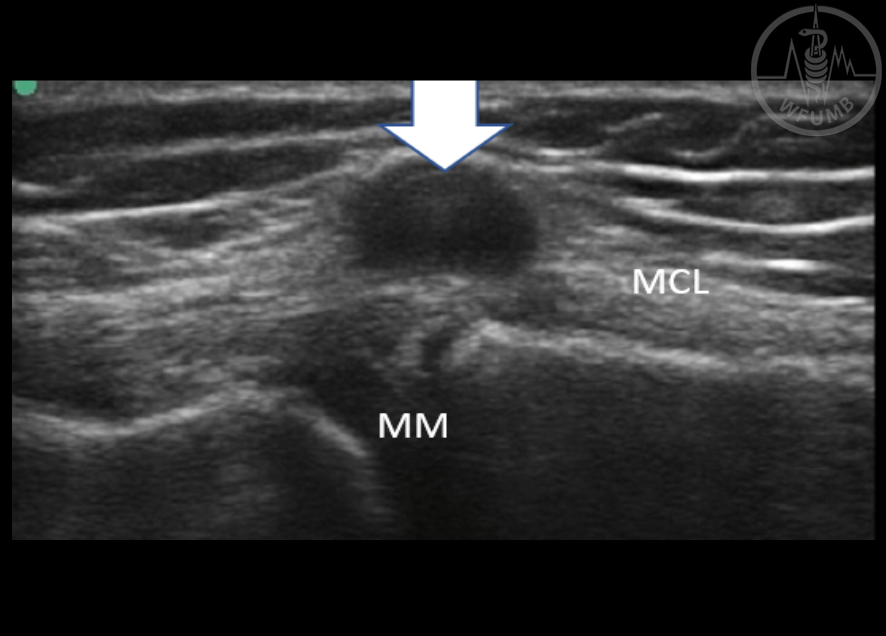
Fig 24.24
Meniscal cyst (Knee). Anechoic non-compressible mass visualized medial to the medial meniscus (MM) (MCL: medial collateral ligament)
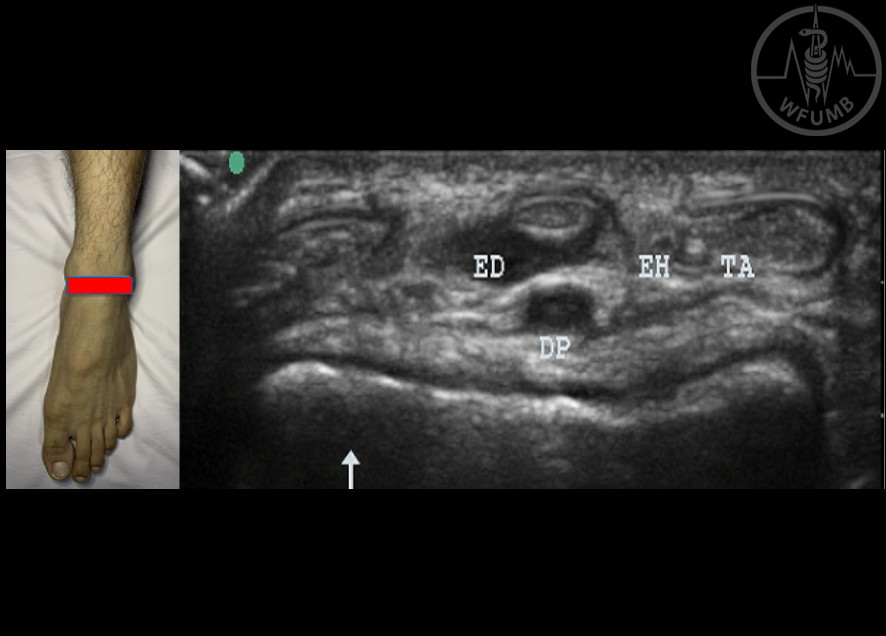
Fig 24.25a
Ankle and foot scanning protocol - anterior ankle in short axis (SAX). Position: patient seated, knees flexed to 45 degrees and ankle in plantar flexion or foot flat on the table (TA: Tibialis Anterior, EH: Extensor Hallucis Longus, ED: Extensor Digitorum Longus, DP: Dorsalis pedis)
Fig 24.25b
Ankle and foot scanning protocol - anterior ankle (anterior recess) in long axis (LAX). Legend: red arrow: Anterior ankle joint recess
Fig 24.26
Partial tear of anterior talofibular ligament (ankle). White arrow: Anechoic-hypoechoic partial disruption of the ligament
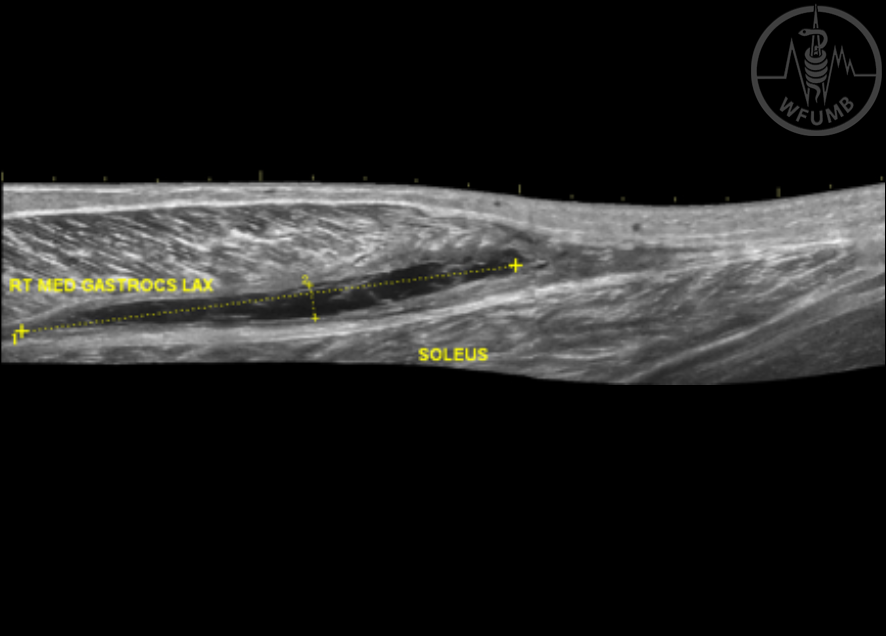
Fig 24.27
Medial gastrocnemius muscle rupture (Ankle). Anechoic fiber disruption of the medial gastrocnemius muscle at the myotendinous junction
Fig 24.28
Achilles tendon rupture (Ankle). Complete anechoic discontinuity of the fibrillar pattern of the tendon (white arrow)
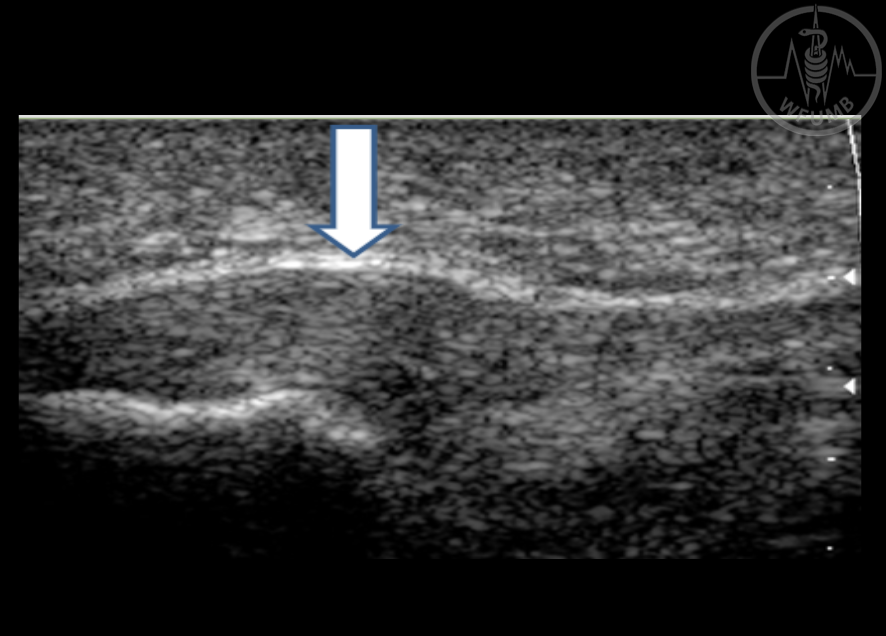
Fig 24.29
Plantar fasciitis (Foot). Hypoechoic thickening o the proximal part of the fascia (White arrow)
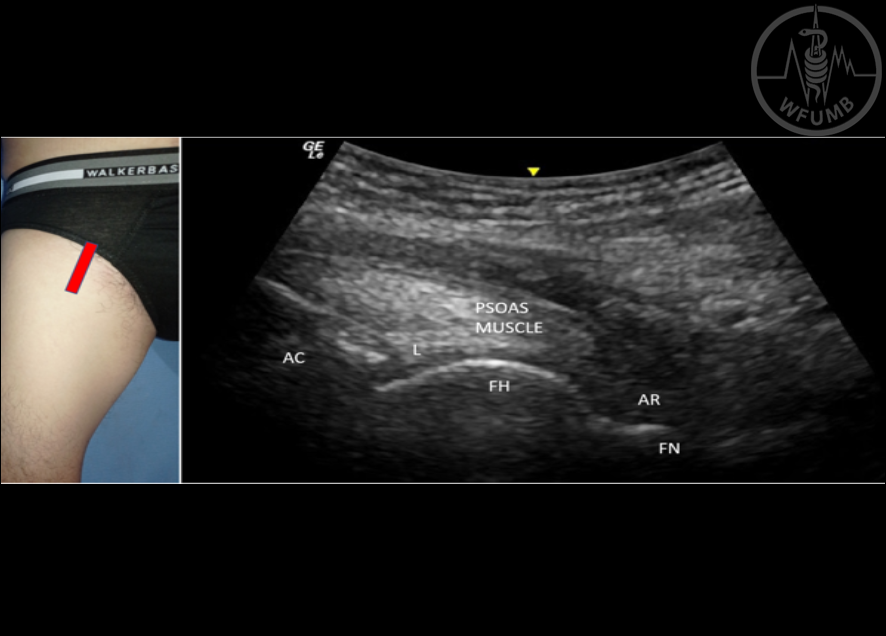
Fig 24.30a Hip scanning protocol - anterior hip.
Position: Place the transducer in oblique longitudinal plane over the femoral neck to identify and evaluate the anterior synovial recess, using the femoral head as land mark. Moving transducer cranially you will identify the homogenous triangular anterior labrum and acetabulum (AC: Acetabulum, FH: Femoral head, L: Anterior Labrum, AR: Anterior recess, FN: Femoral neck)
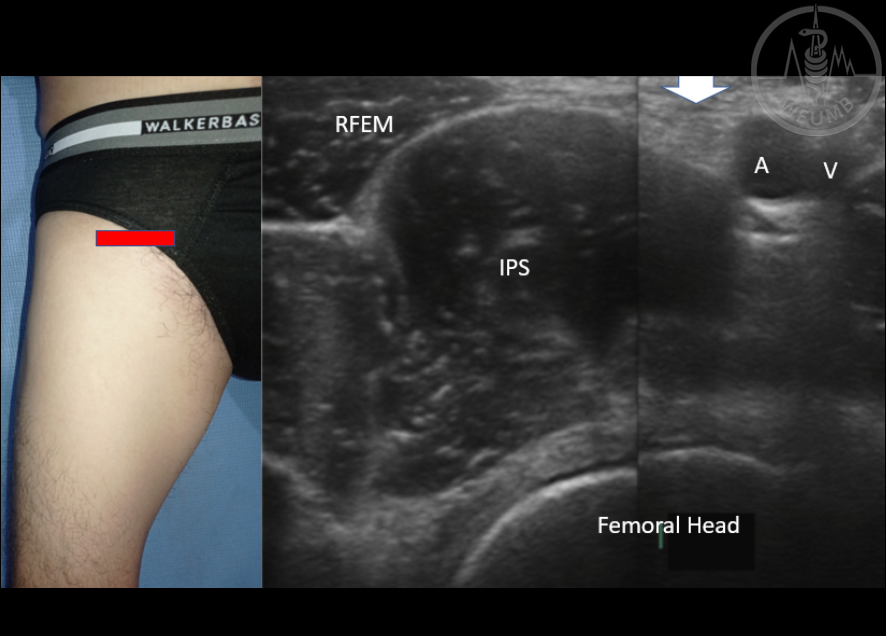
Fig 24.30b Hip scanning protocol - anterior hip.
Position: Place the probe in the transverse plane. Over the joint space and femoral head, you will identify the iliopsoas muscle, lateral to femoral neurovascular bundle (RFEM: Rectus femoris muscle, IPS: Iliopsoas muscle, White arrow: Femoral Nerve, A: Femoral artery, V: Femoral vein)