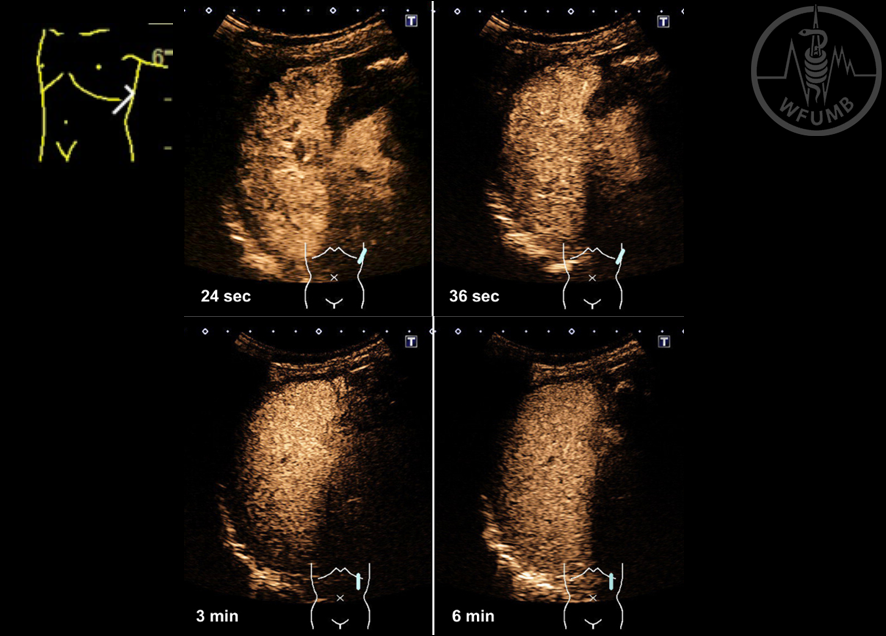
Fig 16.1
Contrast-enhanced US of the spleen: inhomogeneous enhancement in the early arterial phase (24 seconds after intravenous injection of SonoVue®), homogeneous intense enhancement in the late arterial phase (36 seconds), parenchymal phase (3 minutes); Persistent late-phase enhancement (6 minutes)
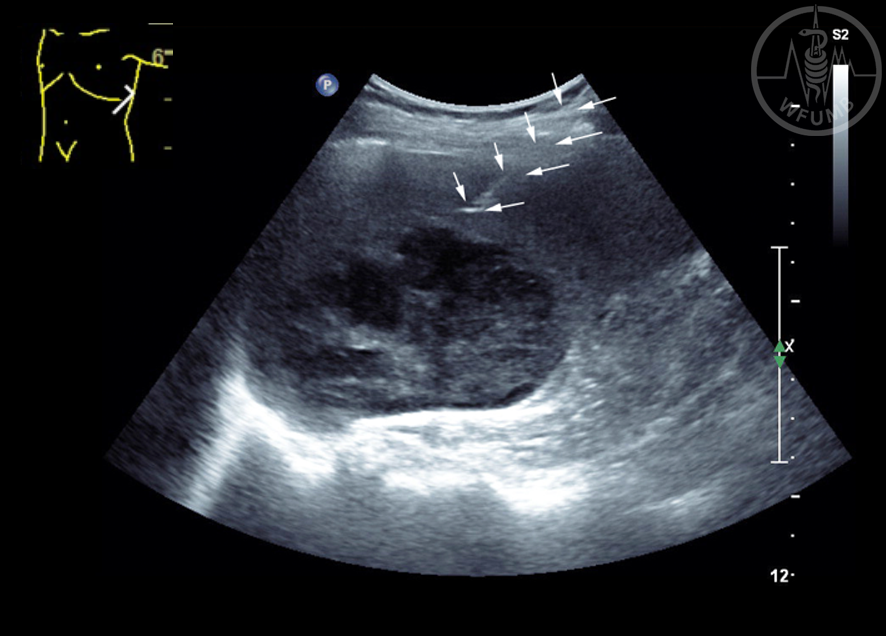
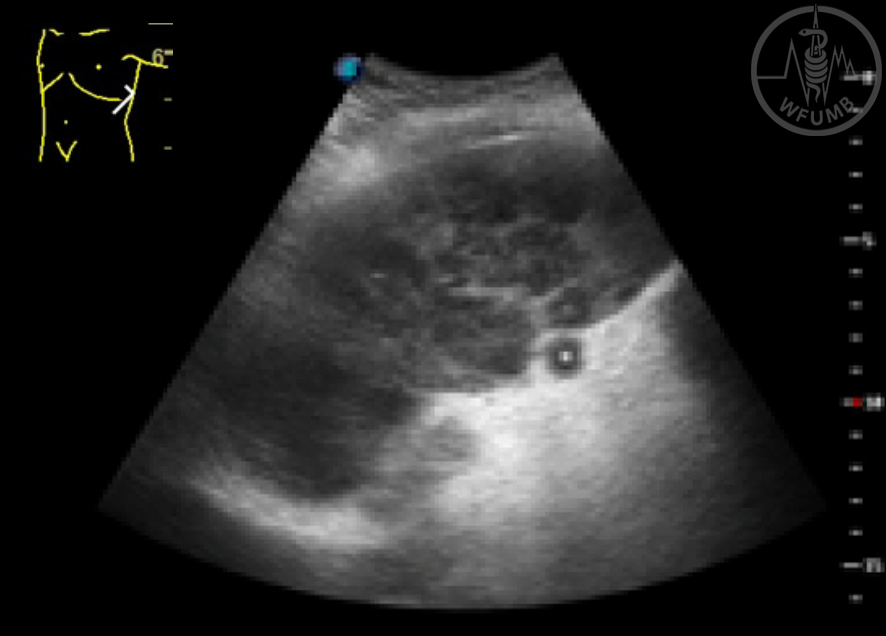
Fig 16.2a
US-guided biopsy of a large hypoechoic and inhomogeneous focal splenic lesion, histologic diagnosis was aggressive non-Hodgkin’s lymphoma
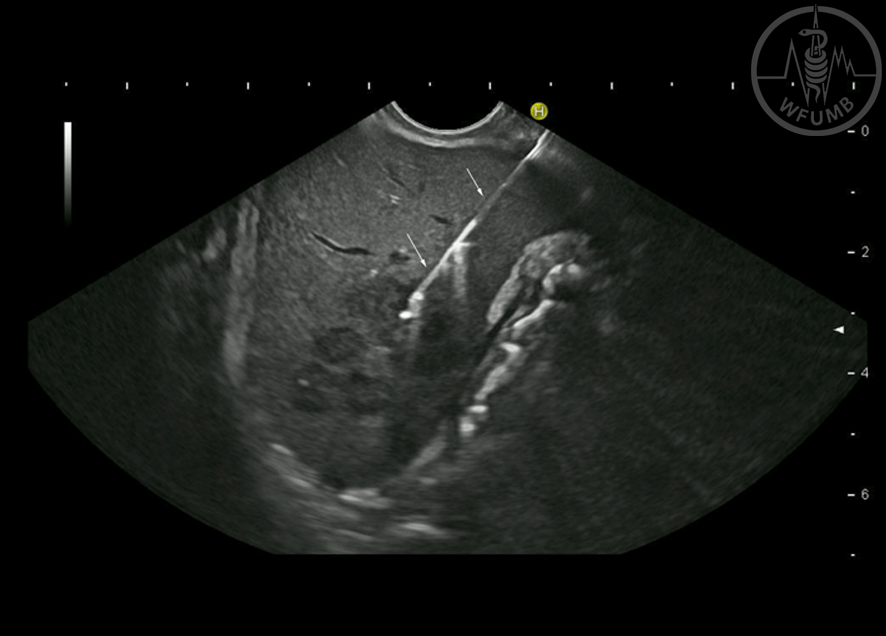
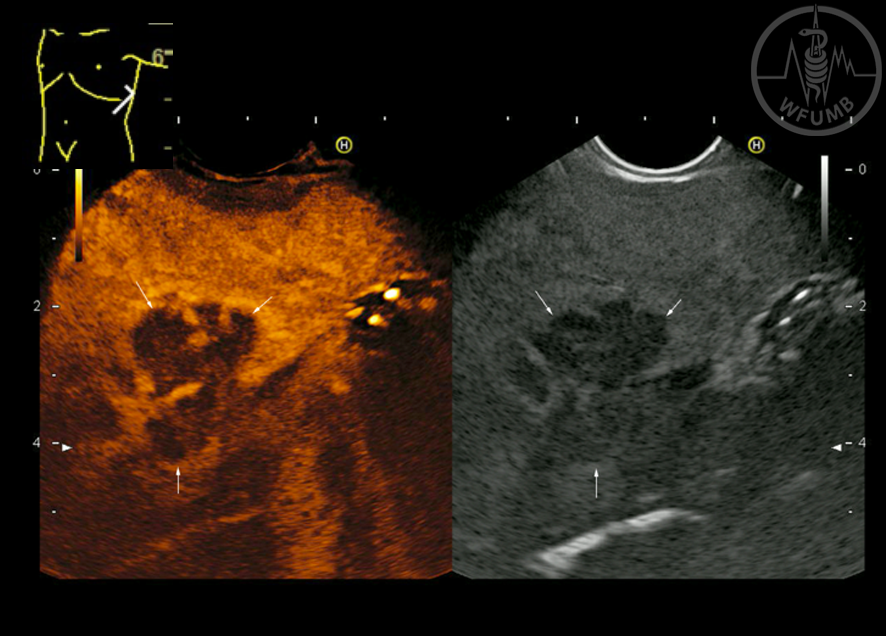
Fig 16.2b
EUS-guided biopsy (22 Gauge) of a large hypoechoic, ill-defined heterogeneous focal lesion in a patient after gastrectomy for gastric cancer, histology revealed metastatic infiltration by signet-cell cancer
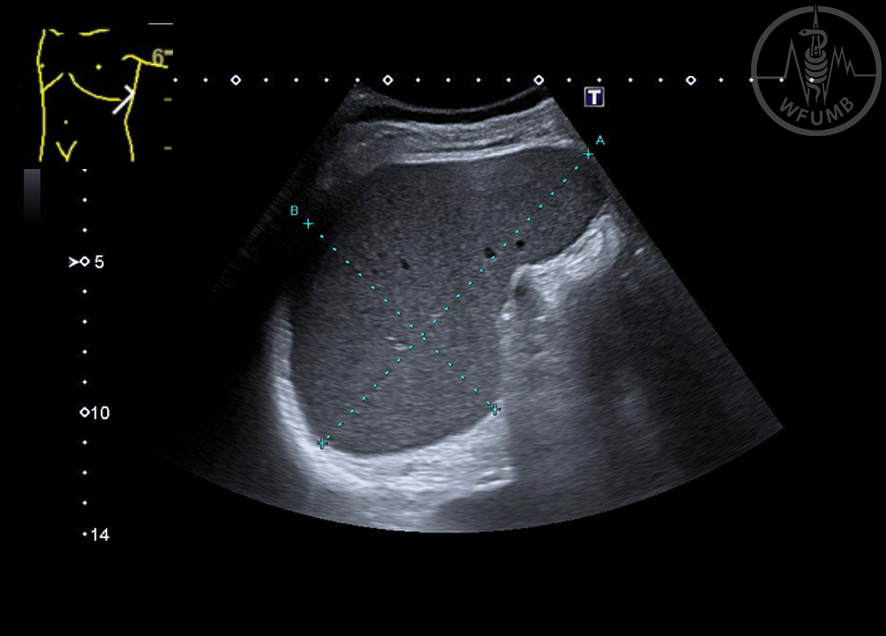
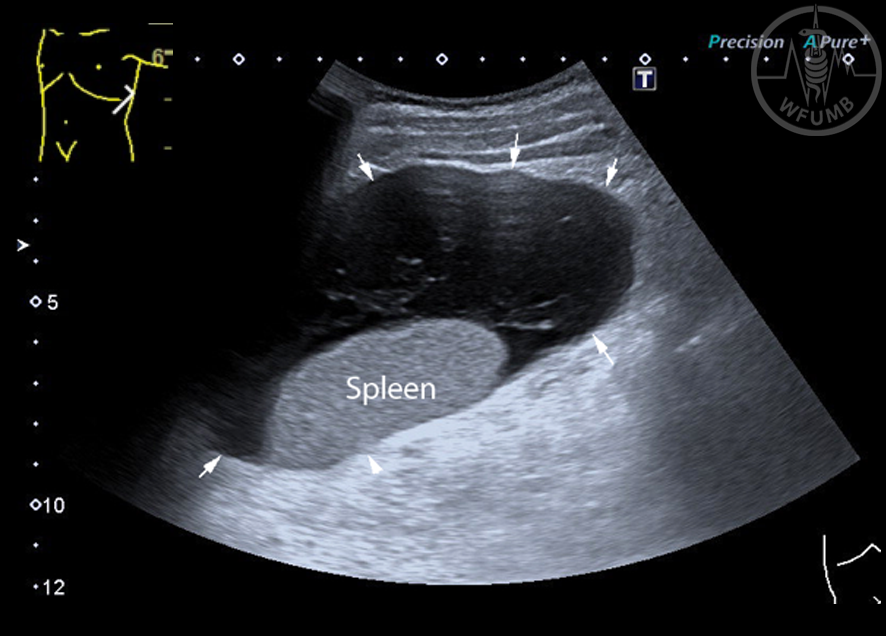
Fig 16.3
Moderately enlarged spleen (13 x 8.7 cm) in a patient with pre-hepatic portal hypertension due to splenic vein thrombosis following acute pancreatitis
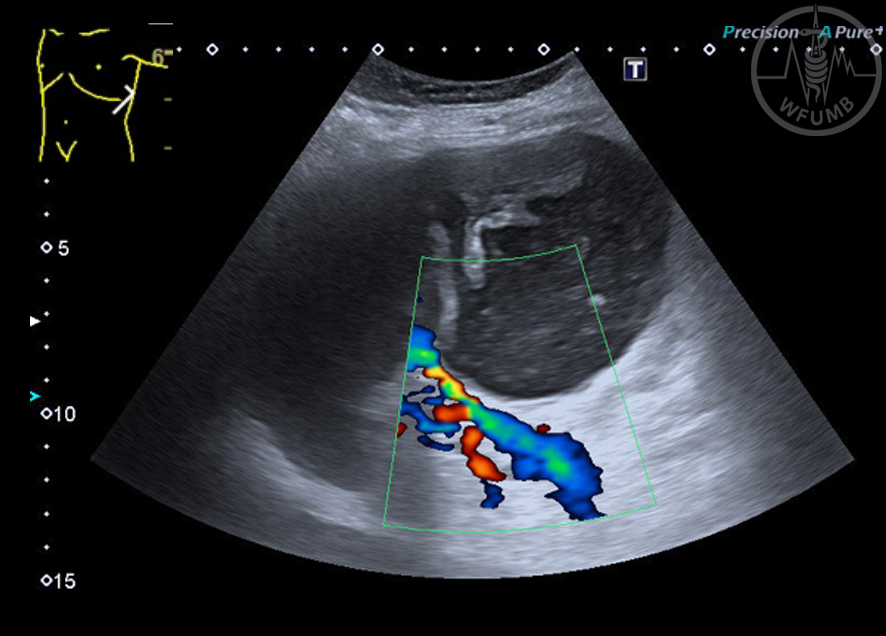
Fig 16.4
Accessory spleen: typical location in the splenic hilum, hilar vessel (Colour Doppler US using Superb Microvascular Imaging Mode)
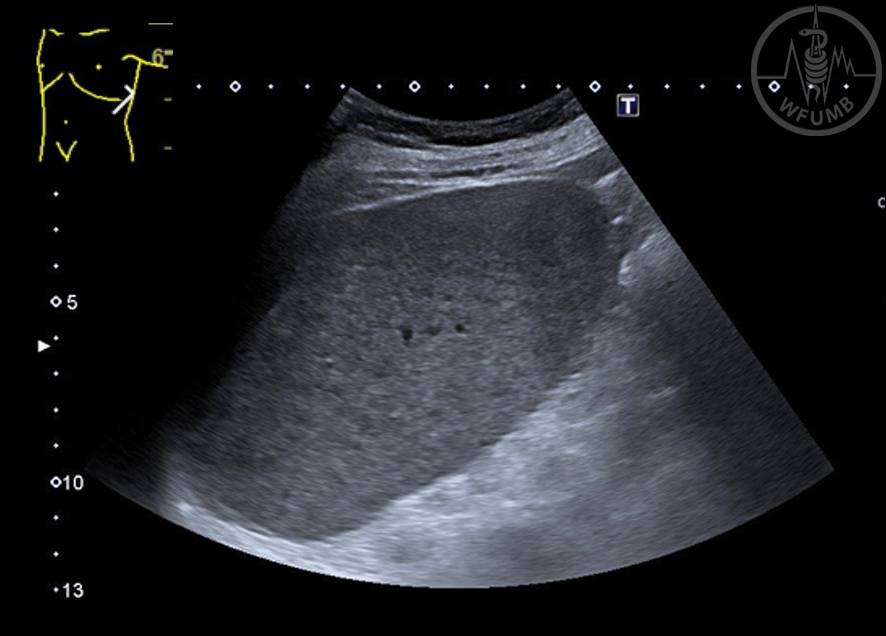
Fig 16.5a
Slightly enlarged spleen with inhomogeneous echotexture in a patient with chronic lymphocytic leukaemia: inhomogeneous echotexture on B-Mode US
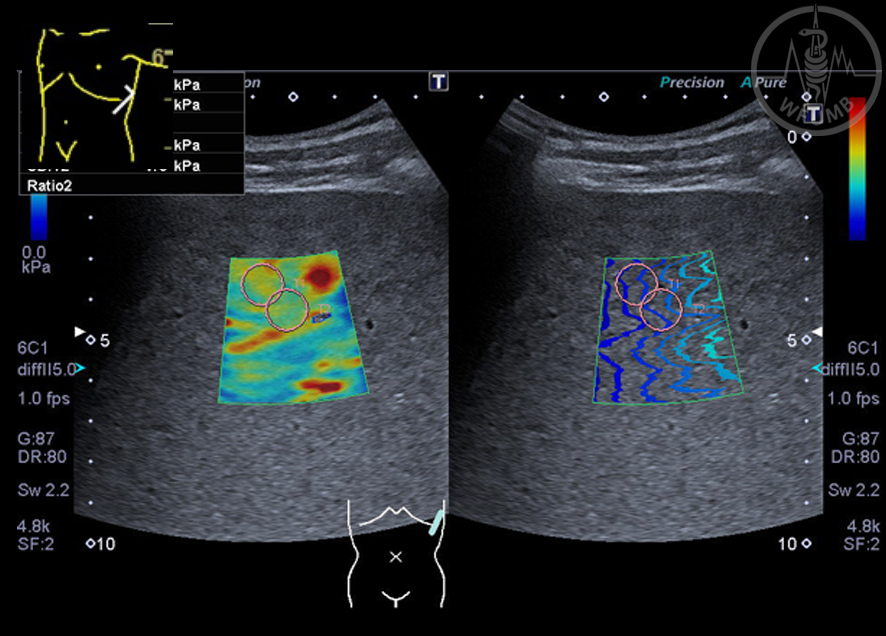
Fig 16.5b
Slightly enlarged spleen with inhomogeneous echotexture in a patient with chronic lymphocytic leukaemia: high stiffness of the splenic parenchyma on shear wave elastography (23 – 25 kPa)
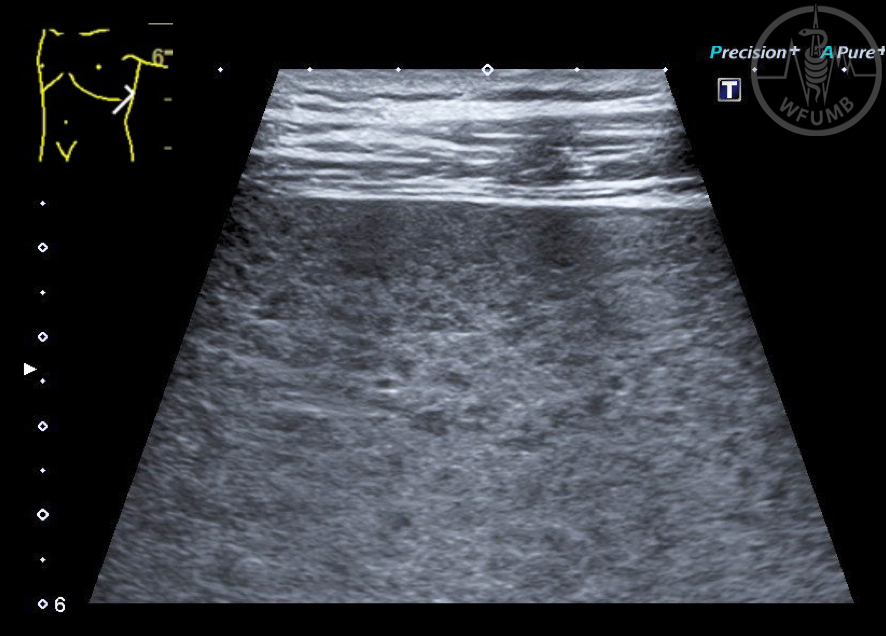
Fig 16.5c
Slightly enlarged spleen with inhomogeneous echotexture in a patient with chronic lymphocytic leukaemia: hypoechoic micronodularity on high frequency US (3 - 11 MHz)
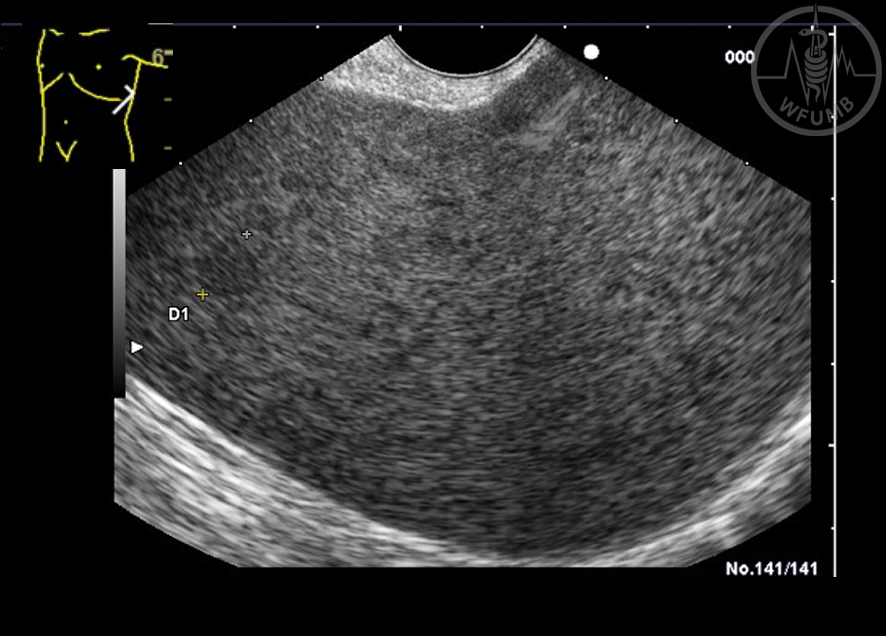
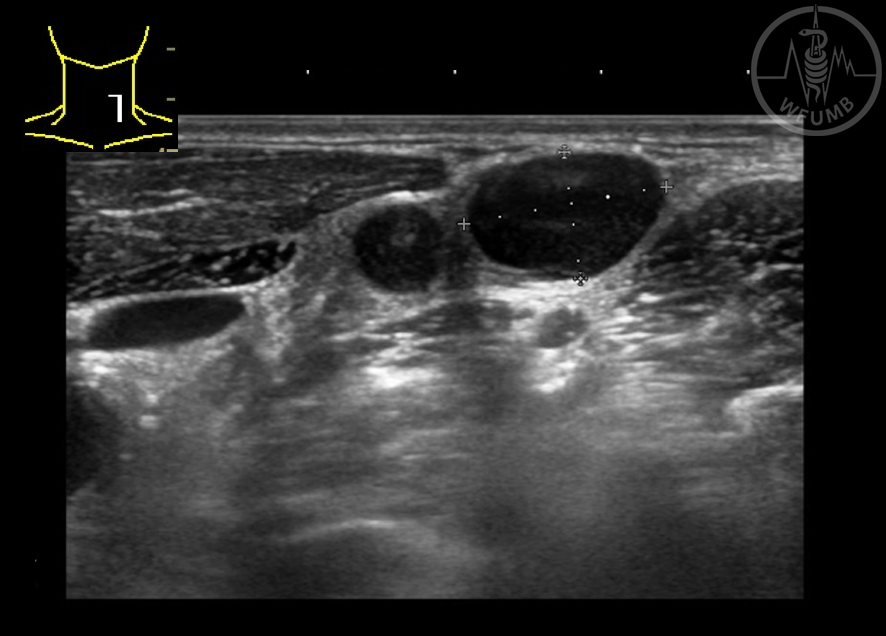
Fig 16.5d
Slightly enlarged spleen with inhomogeneous echotexture in a patient with chronic lymphocytic leukaemia: small hypoechoic nodular lesions (2 mm - 9 mm, between markers) on high-frequency endoscopic ultrasound (7.5 MHz)
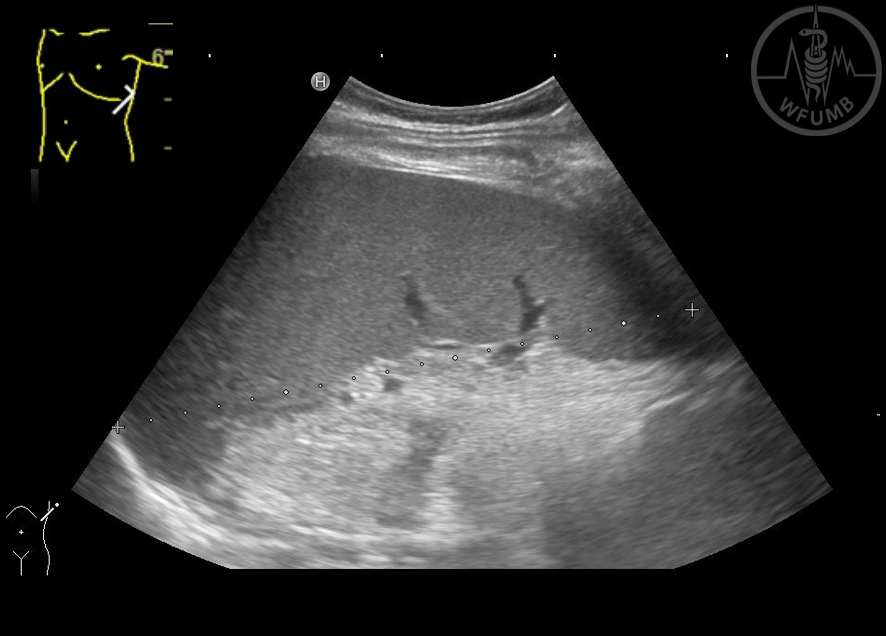
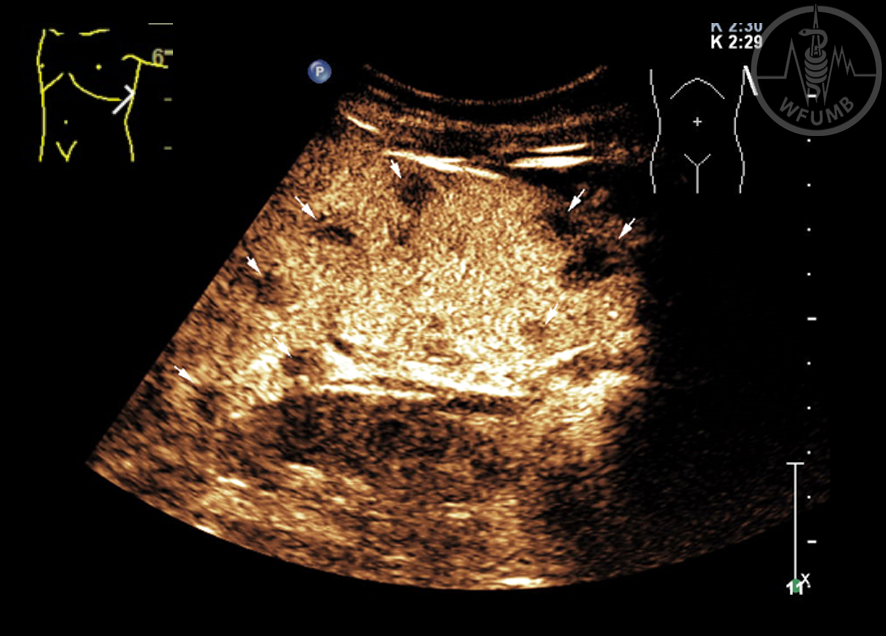
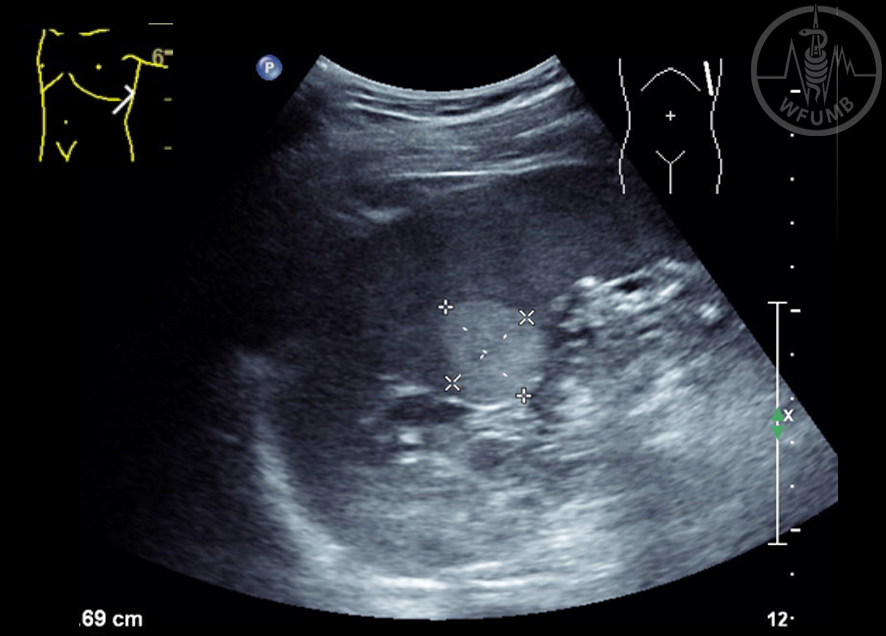
Fig 16.6a
Moderately enlarged spleen (17 x 7 cm) in a patient with infectious mononucleosis and left flank pain
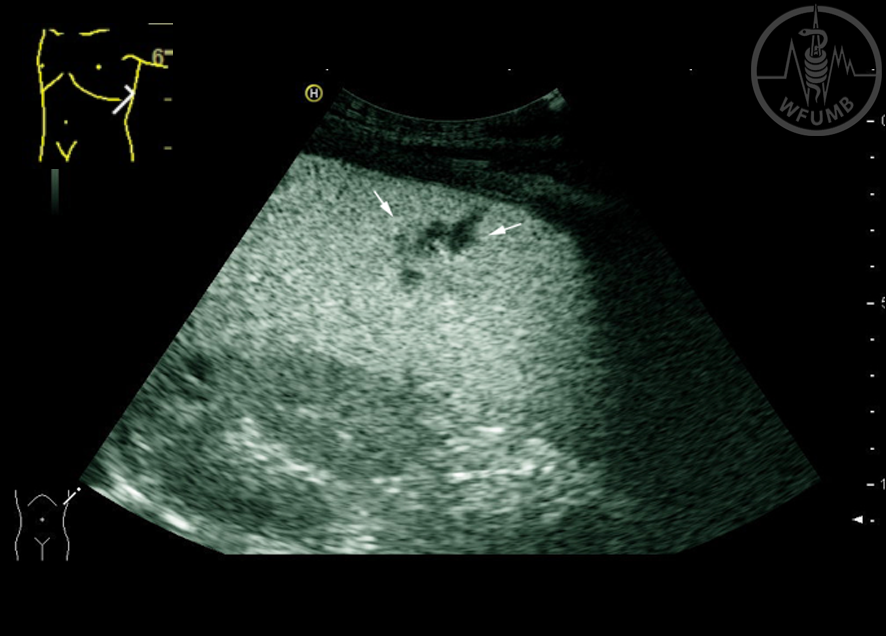
Fig 16.6b
Moderately enlarged spleen (17 x 7 cm) in a patient with infectious mononucleosis and left flank pain. Detailed examination reveals a small parenchymal inhomogeneity (arrows)
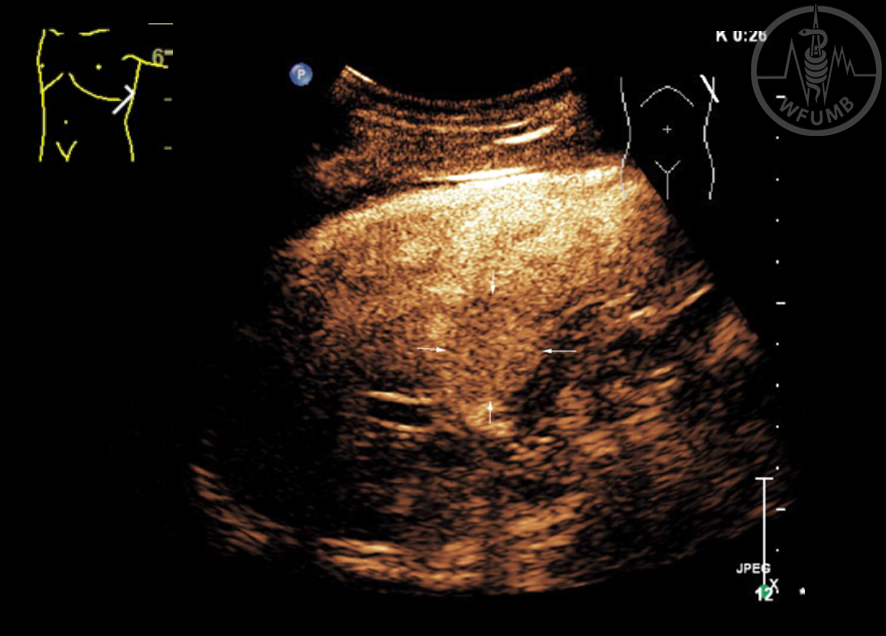
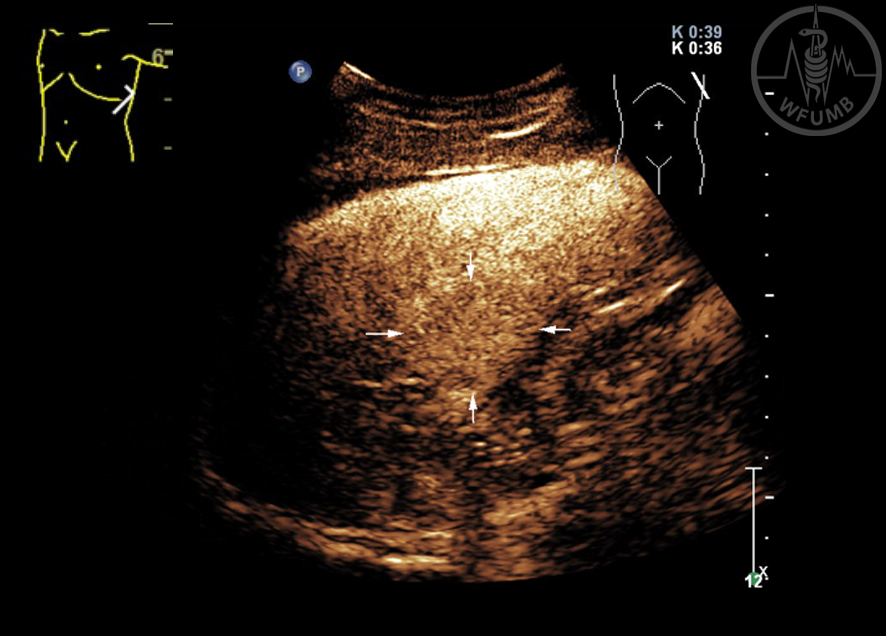
Fig 16.6c
Moderately enlarged spleen (17 x 7 cm) in a patient with infectious mononucleosis and left flank pain. CEUS shows focal non-enhancement in this small area, suggestive for a small parenchymal laceration (90 seconds after injection of the US contrast agent SonoVue®)
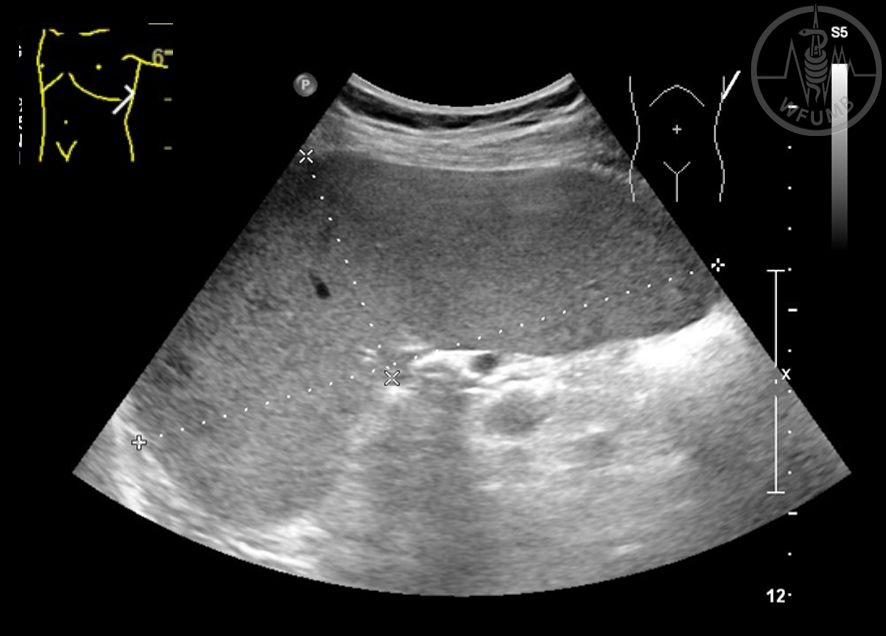
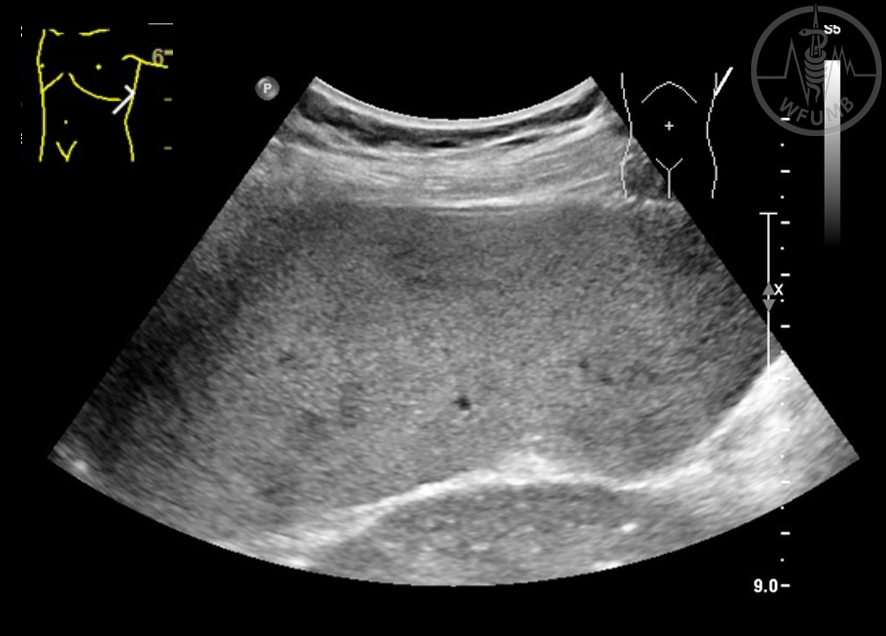
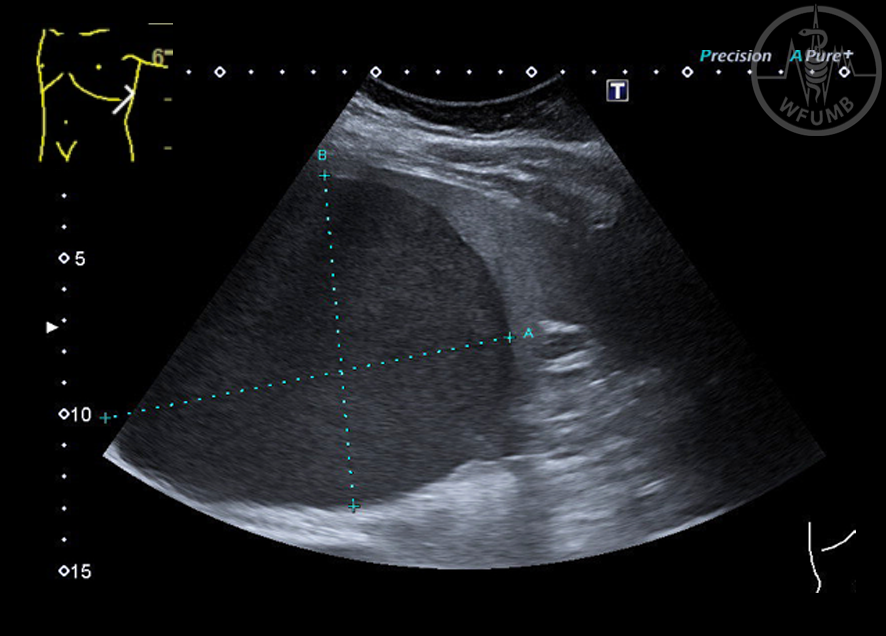
Fig 16.7a
Splenomegaly, incidental finding (15 x 6 cm)
Fig 16.7b
Splenomegaly, incidental finding (15 x 6 cm). A closer view reveals parenchymal inhomogeneities
Fig 16.7c
Splenomegaly, incidental finding (15 x 6 cm). CEUS showed multiple non-enhancing focal lesions (parenchymal phase). EUS-guided fine-needle sampling of mediastinal lymph nodes resulted in diagnosis of sarcoidosis
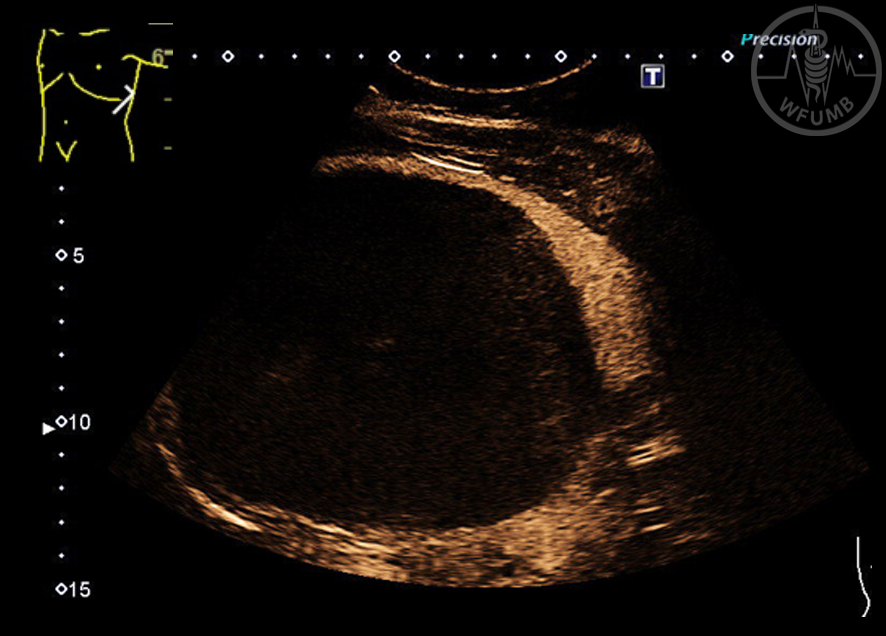
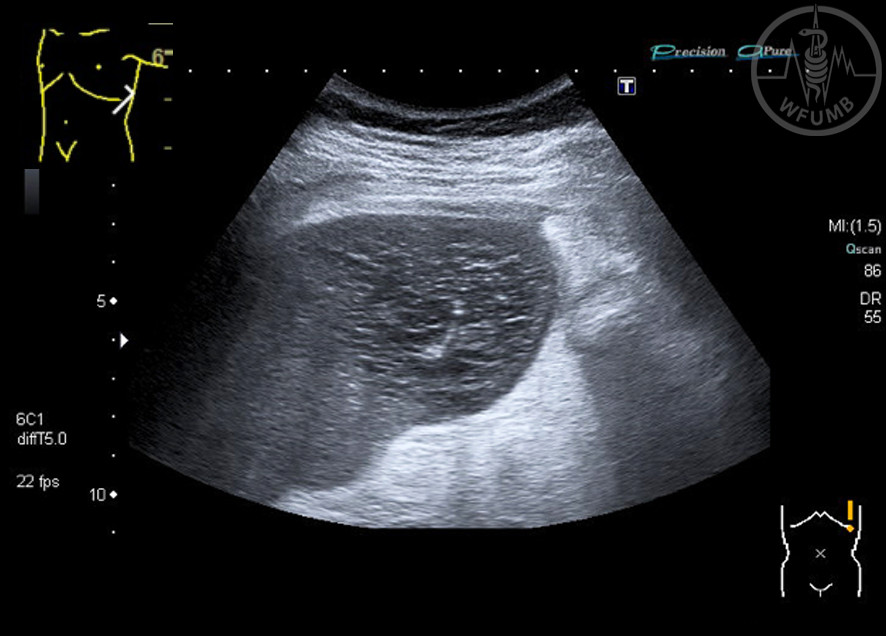
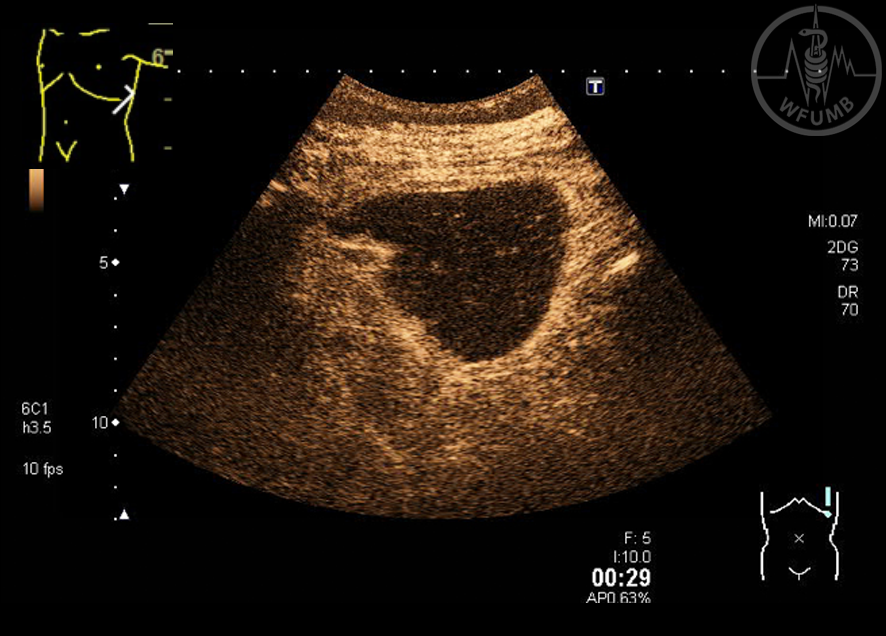
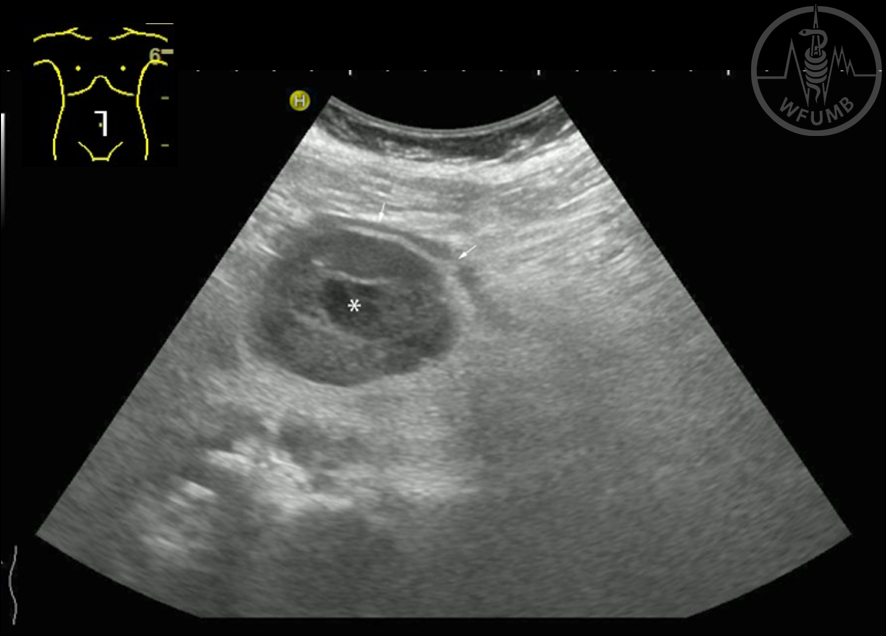
Fig 16.8a
Large splenic (pseudo-)cyst (13.2 x 10.6 cm, between markers) in a patient several years after blunt abdominal trauma. On B-Mode US the lesion appears hypoechoic
Fig 16.8b
Large splenic (pseudo-)cyst (13.2 x 10.6 cm, between markers) in a patient several years after blunt abdominal trauma. Cystic nature is proven by CEUS (no enhancement)
Fig 16.9a
Intrasplenic pancreatic pseudocysts: large fluid collection of the lower half of the spleen with echogenic reflexes and without any enhancement (B-Mode)
Fig 16.9b
Intrasplenic pancreatic pseudocysts: large fluid collection of the lower half of the spleen with echogenic reflexes and without any enhancement (CEUS)
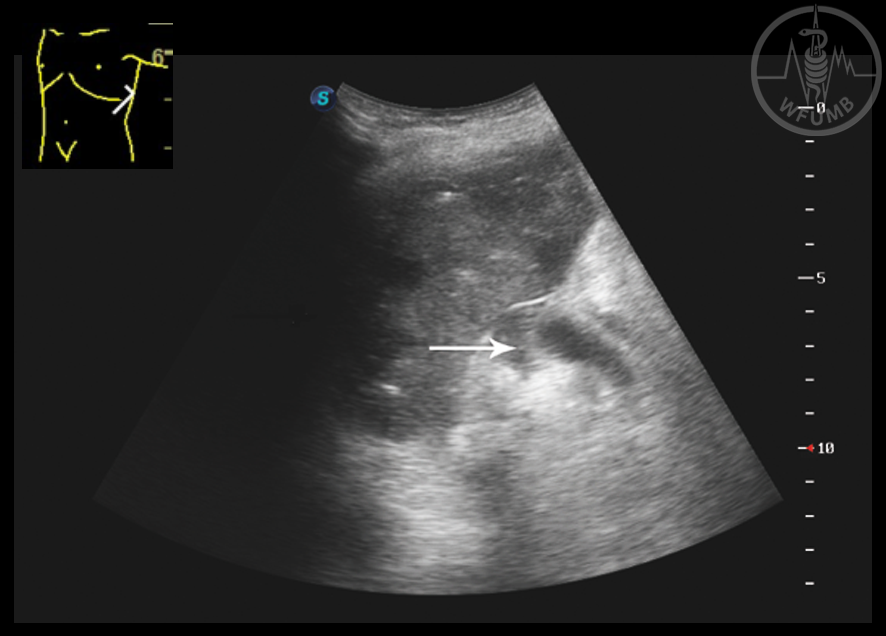
Fig 16.9c
Intrasplenic pancreatic pseudocysts: large fluid collection within the splenic capsule (marked with arrows), the splenic parenchyma is compressed
Fig 16.10b
Hyperechoic splenic lesion. On CEUS (early arterial phase) the lesion is isoenhancing (arrows), indicating a benign vascular tumor, e.g. hemangioma
Fig 16.10c
Hyperechoic splenic lesion. On CEUS (late phase) the lesion is isoenhancing (arrows), indicating a benign vascular tumor, e.g. hemangioma
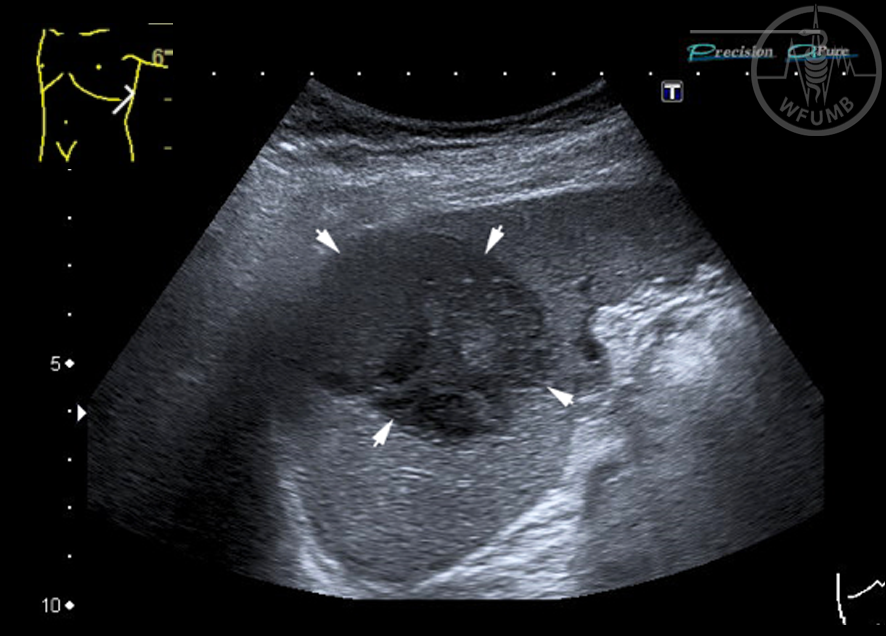
Fig 16.11a
Non-Hodgin’s lymphoma of the spleen. B-Mode US shows a large hypoechoic and inhomogeneous mass lesion (arrows)
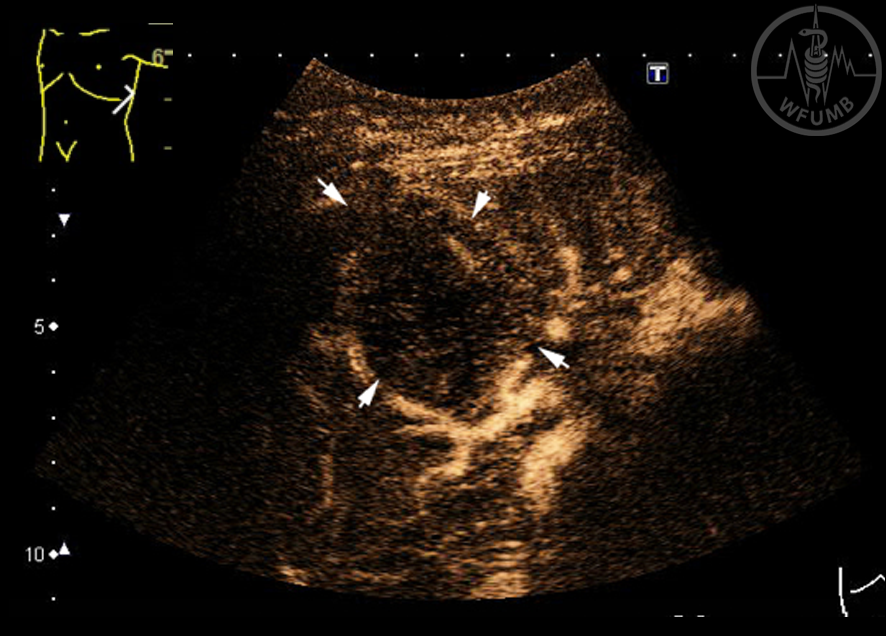
Fig 16.11b
Non-Hodgin’s lymphoma of the spleen. On CEUS the malignant etiology is obvious: in the arterial phase (17 seconds after injection of the US contrast agent SonoVue®) the focal lesion is hypoenhancing
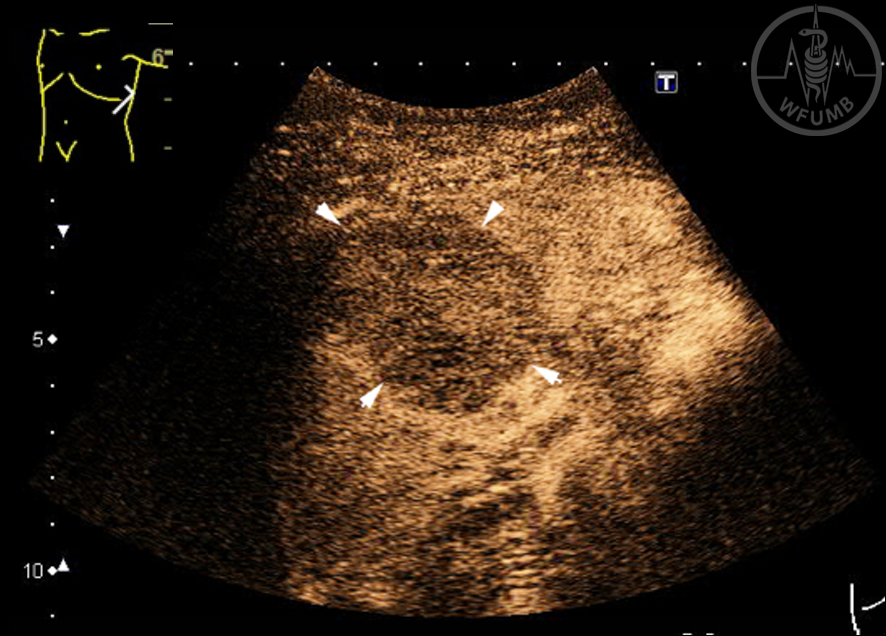
Fig 16.11c
Non-Hodgin’s lymphoma of the spleen. On CEUS the malignant etiology is obvious: in the arterial phase (31 seconds after injection of the US contrast agent SonoVue®) the focal lesion is hypoenhancing)
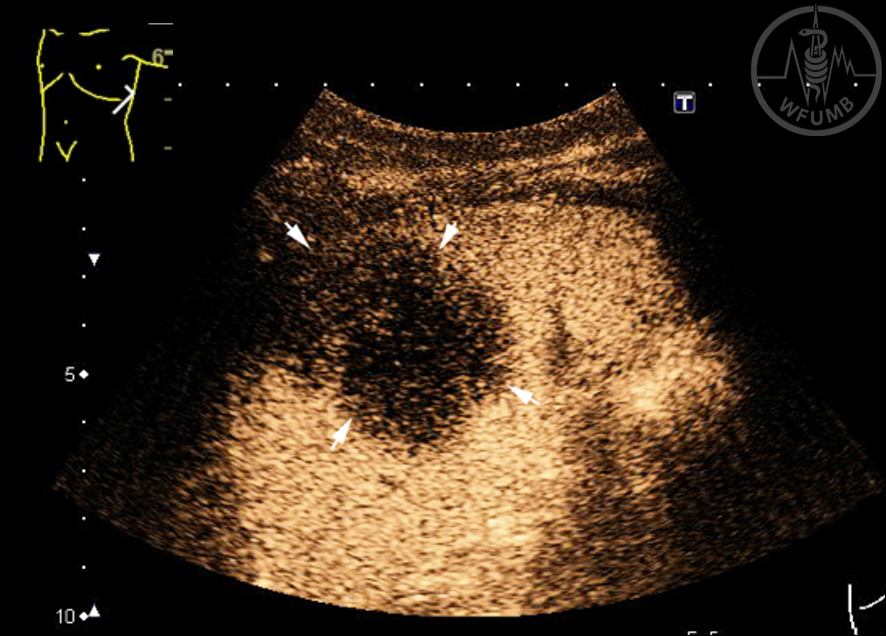
Fig 16.11d
Non-Hodgin’s lymphoma of the spleen. On CEUS the malignant etiology is obvious: distinct late-phase washout (212 seconds after injection) is occurring
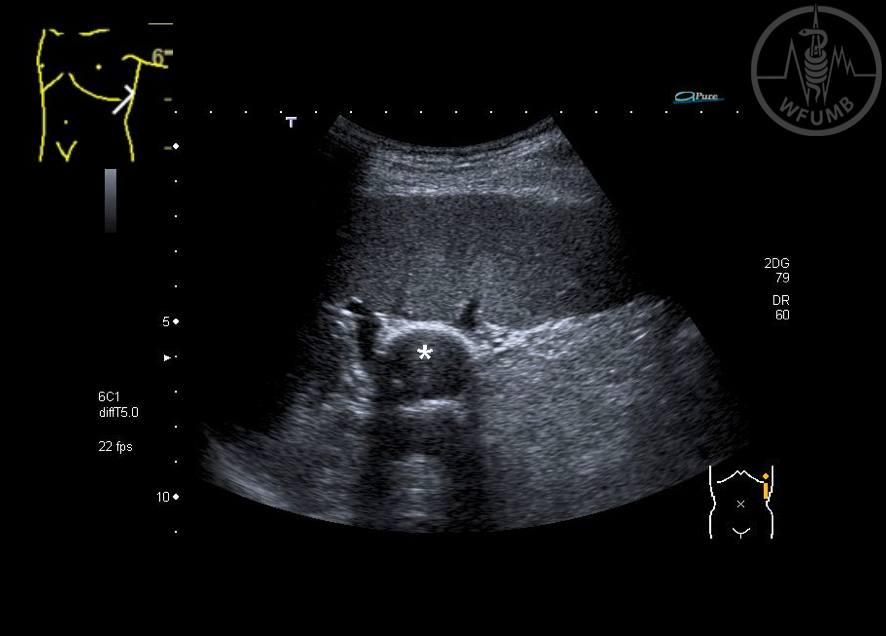
Fig 16.12
Multiple hypoechoic focal splenic lesions and a hilar perisplenic lymph node (*) in a patient with non-Hodgkin’s lymphoma (B-Mode US)
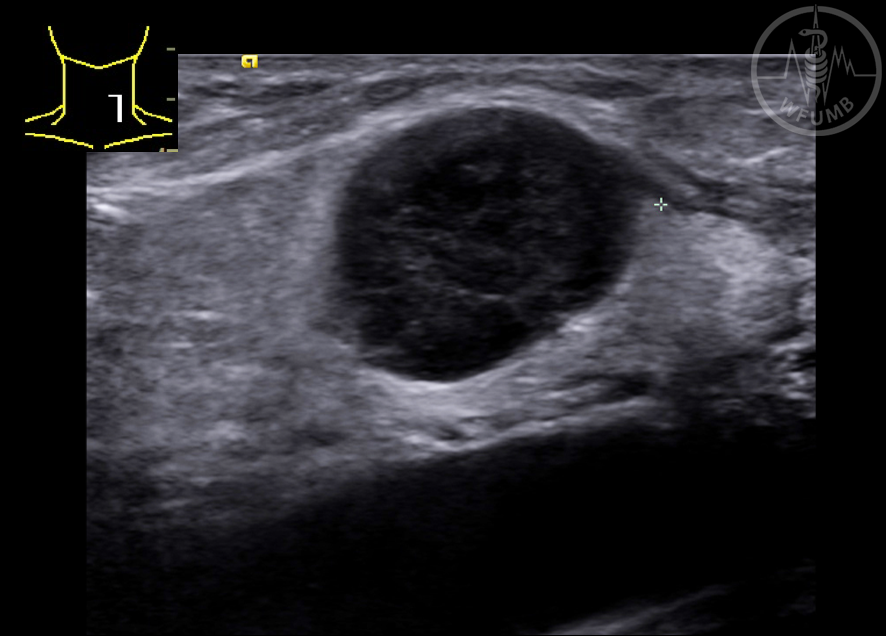
Fig 16.13a
B-Mode US of a hypoechoic and inhomogeneous focal lesion near the splenic hilum in a patient with a history of gastrectomy for cancer. EUS-guided biopsy was performed (Fig. 16.2b)
Fig 16.13b
Contrast-enhanced harmonic of a hypoechoic and inhomogeneous focal lesion EUS shows late-phase hypoenhancement, predicting malignancy. EUS-guided biopsy was performed (Fig. 16.2b)
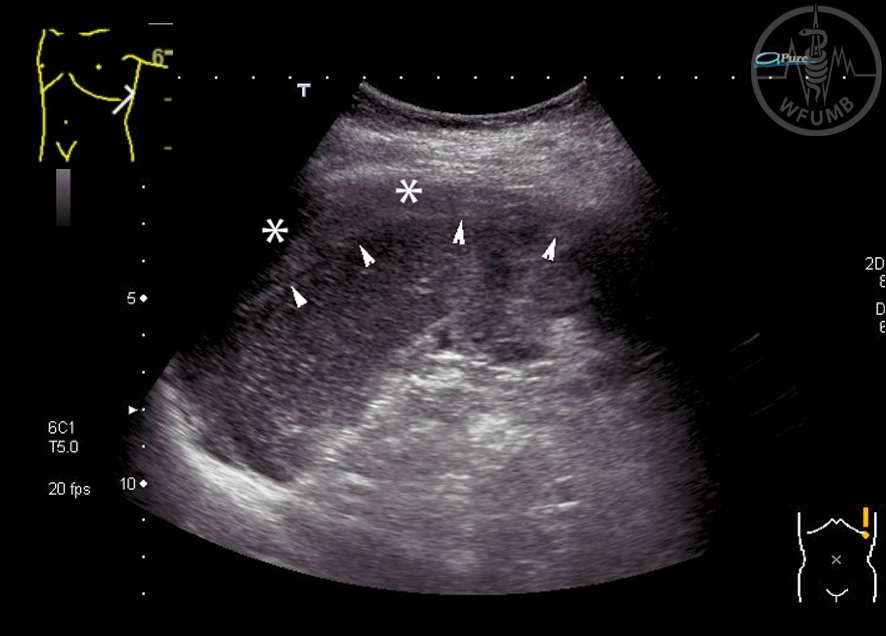
Fig 16.14
Splenic bleeding: Slightly hyperechoic hematoma between spleen and diaphragm (*), the border between splenic parenchyma and hematoma is ill-defined (arrowheads)
Fig 16.15a
B-Mode US in a patient 4 weeks after left flank pain and paroxysmal atrial fibrillation reveals an inhomogeneous area in the region of the lower splenic pole
Fig 16.15b
CEUS in a patient 4 weeks after left flank pain and paroxysmal atrial fibrillation reveals an inhomogeneous area in the region of the lower splenic pole. 29 seconds after injection of the US contrast agent SonoVue® non-enhancement is visible, and diagnosis of splenic infarction is established
Fig 16.16
Complete splenic infarction, no enhancement at all on CEUS
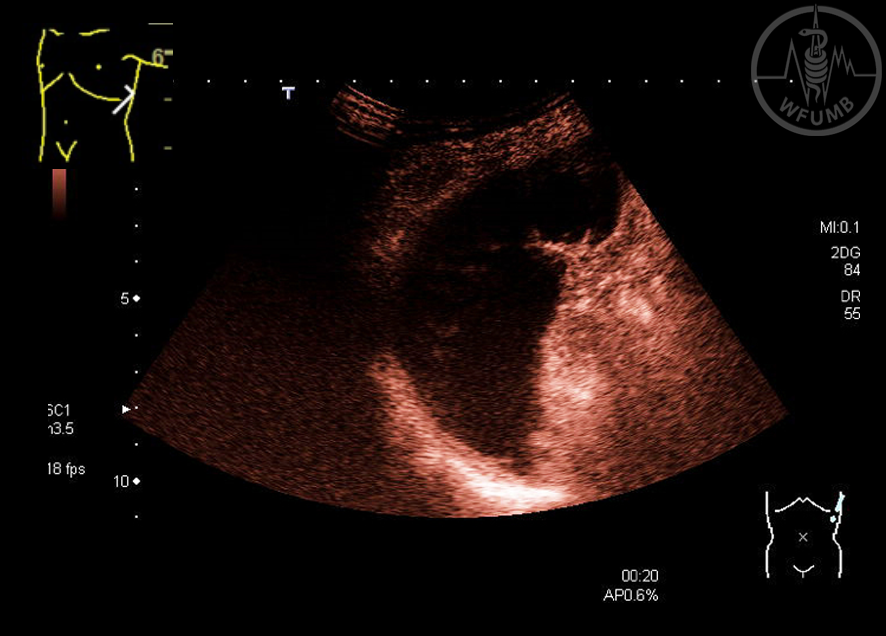
Fig 16.17a
Splenic vein thrombosis and massive splenic necrosis or hematoma after partial splenectomy in a patient with giant splenomegaly due to hereditary microspherocytosis: B-Mode US
Fig 16.17b
Splenic vein thrombosis and massive splenic necrosis or hematoma after partial splenectomy in a patient with giant splenomegaly due to hereditary microspherocytosis: CDUS shows a widened hypoechoic splenic vein (arrow) without flow and an inhomogeneous spleen with hypoechoic ill-defined areas
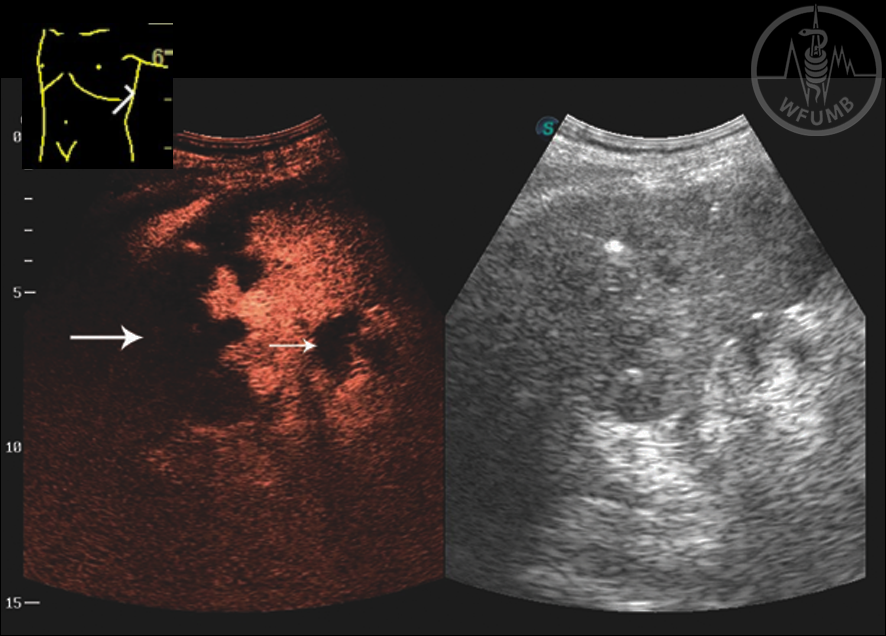
Fig 16.17c
Splenic vein thrombosis and massive splenic necrosis or hematoma after partial splenectomy in a patient with giant splenomegaly due to hereditary microspherocytosis: CEUS (parenchymal phase) proves non-enhancement of large hypoechoic areas within the remaining spleen (large arrow; necrosis or bleeding) and non-enhancement of the splenic vein (small arrow)
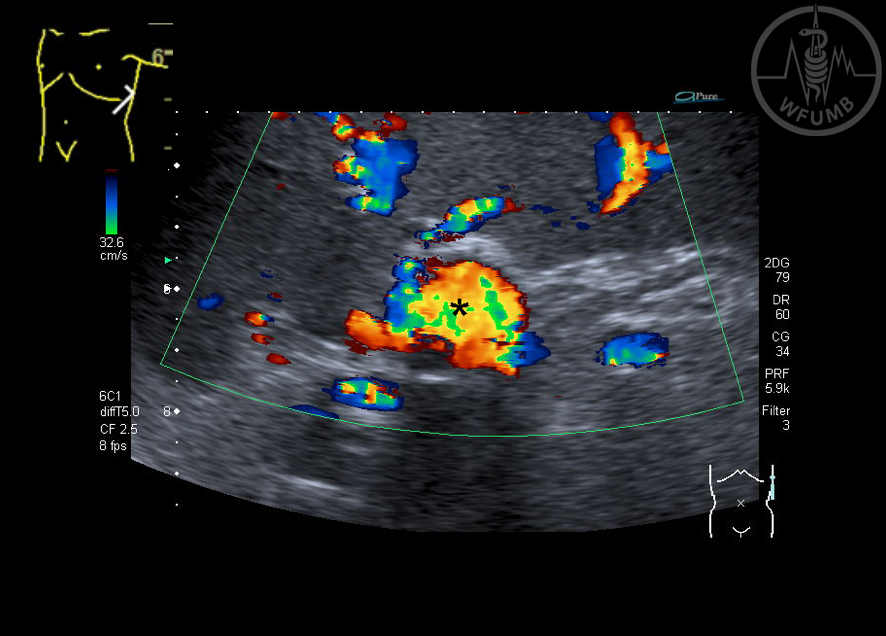
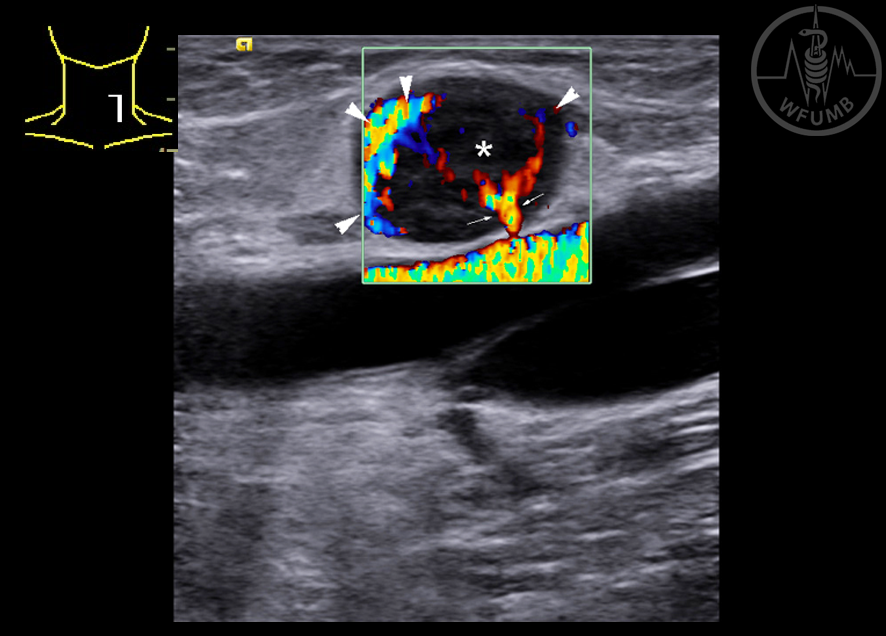
Fig 16.18a
Incidentally detected aneurysm of the splenic artery (*) of unknown etiology, located in the splenic hilum (B-Mode)
Fig 16.18b
Incidentally detected aneurysm of the splenic artery (*) of unknown etiology, located in the splenic hilum (CDUS)
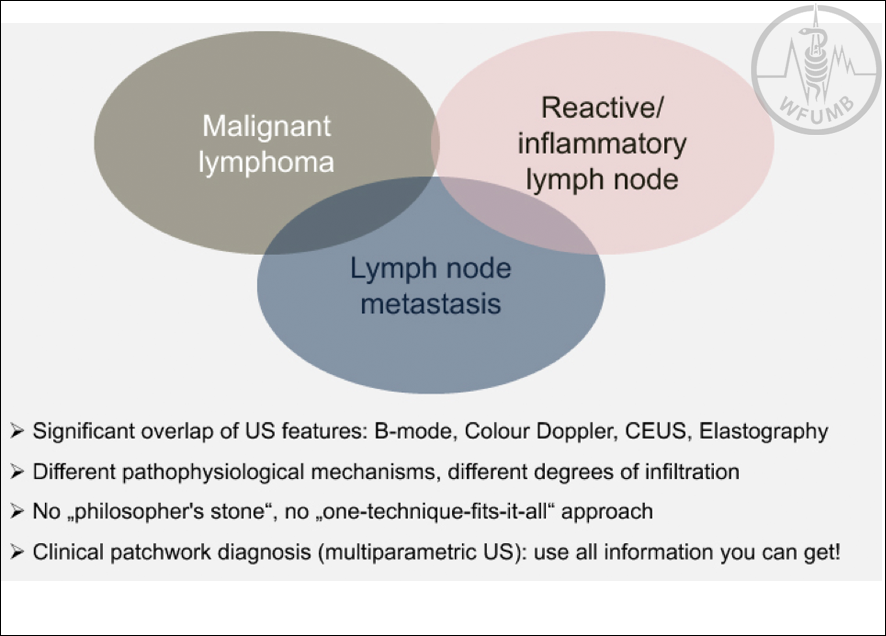
Fig 16.19
Overlap of pathophysiological mechanisms and US features in lymphadenopathy
Fig 16.18b
Incidentally detected aneurysm of the splenic artery (*) of unknown etiology, located in the splenic hilum (CDUS)
Fig 16.19
Overlap of pathophysiological mechanisms and US features in lymphadenopathy
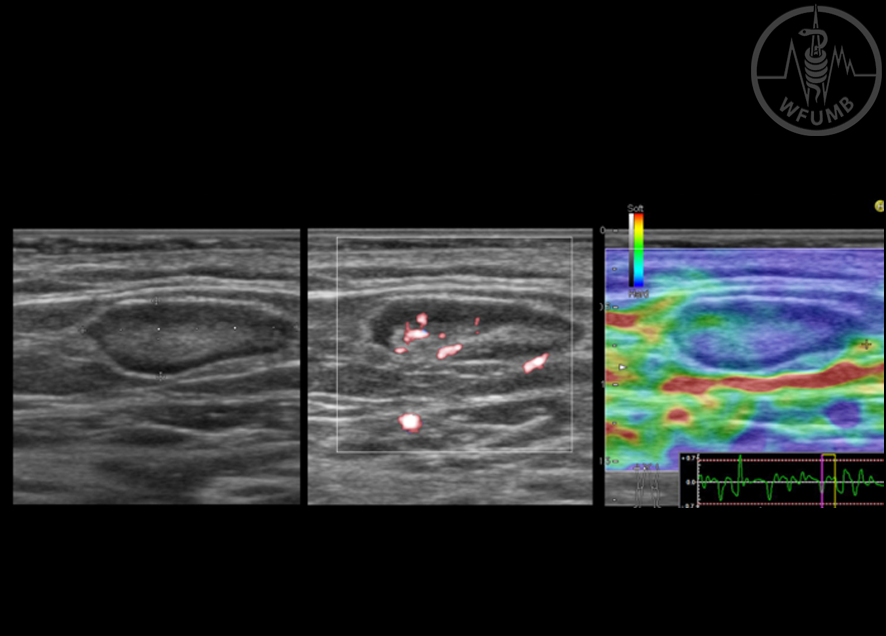
Fig 16.20
Physiological lymph node (peripheral location): flat-oval (14 x 5 mm, Solbiati index 2.8), well-defined small and symmetric hypoechoic cortex, echogenic hilum reflex (B-Mode US), hilar vessels visible on CDUS, on strain elastography the cortex appearing slightly stiffer compared to the hilum
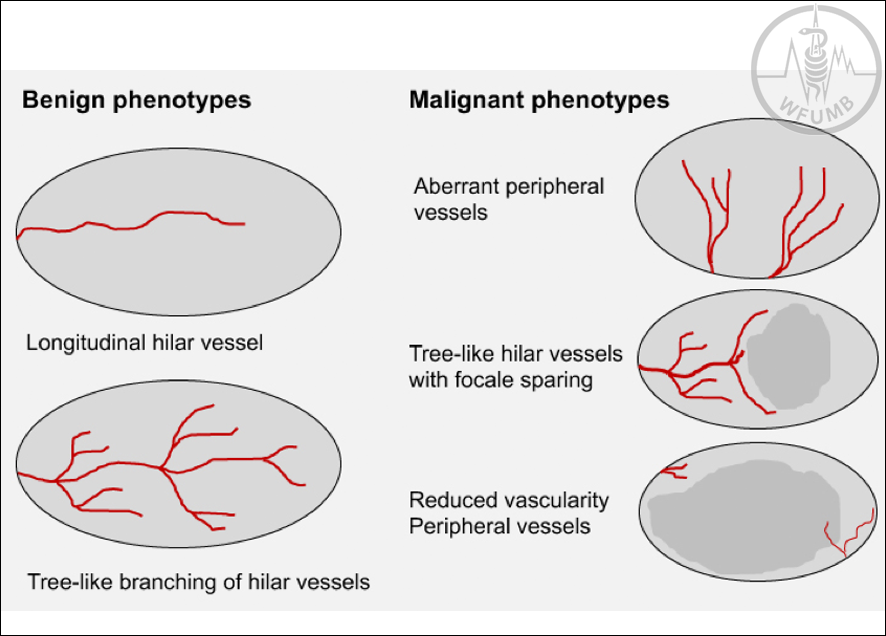
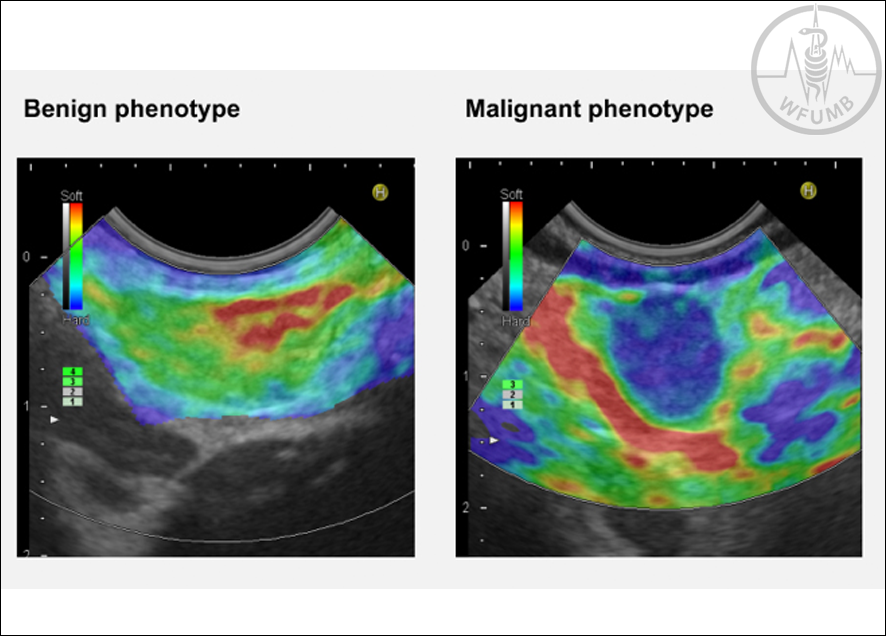
Fig 16.21
Benign and malignant phenotypes of lymph node vascularisation (modified from Tschammler A et al. Radiology 1998; 208; 117-123)
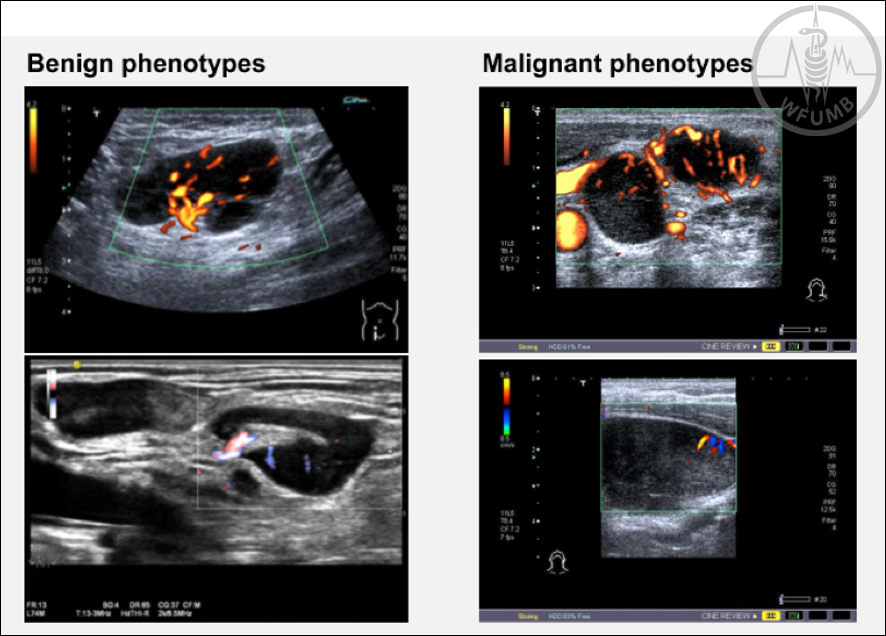
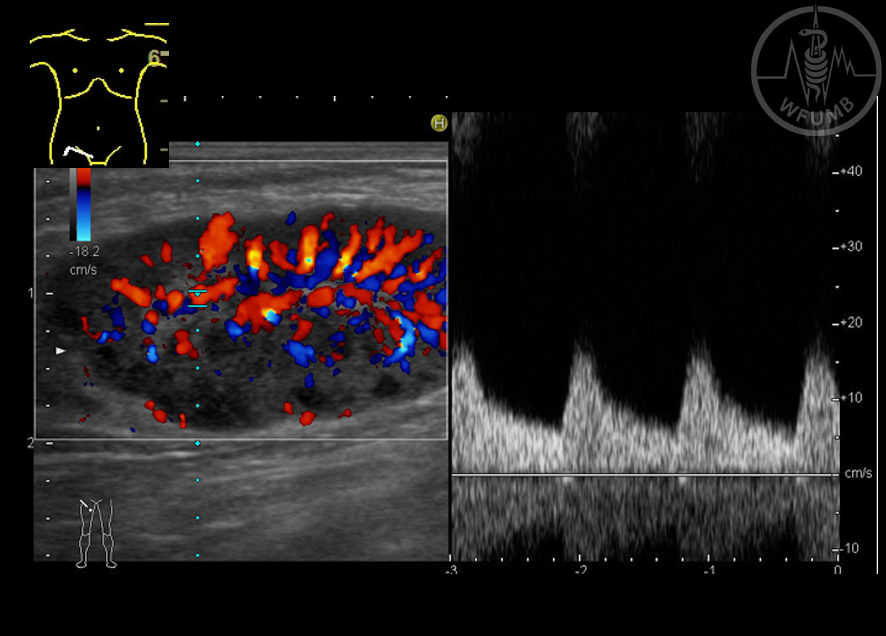
Fig 16.22
Benign and malignant phenotypes of lymph node vascularisation (typical examples)
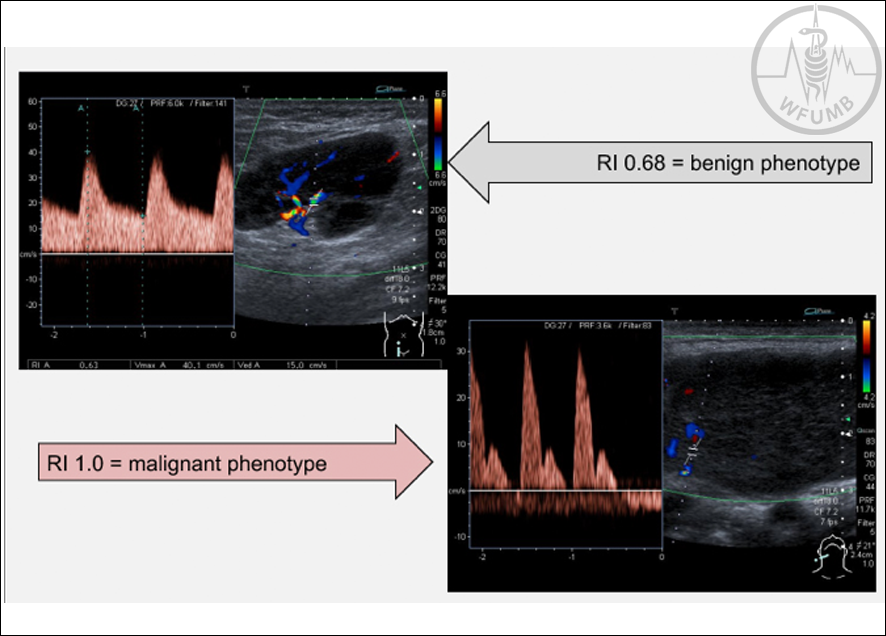
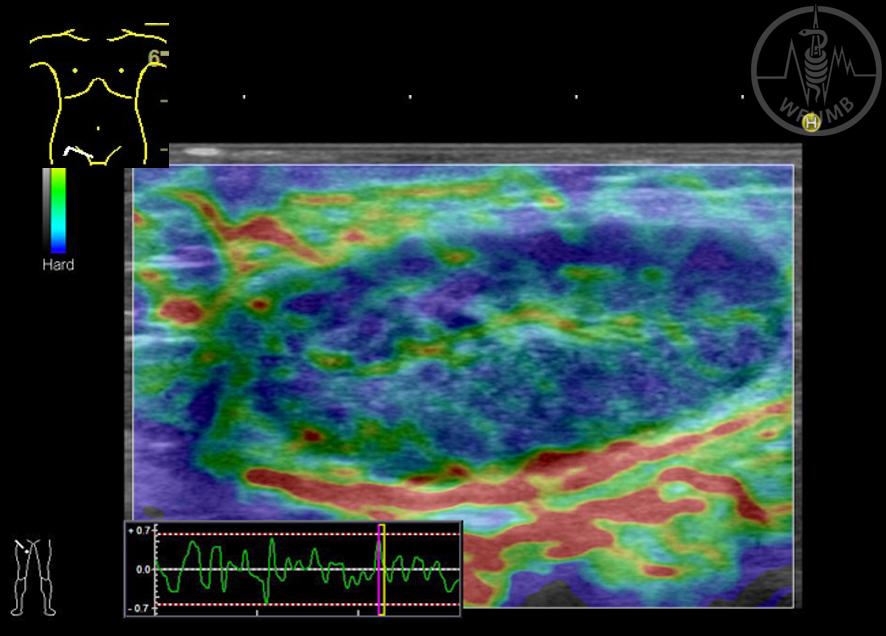
Fig 16.23
Benign and malignant phenotypes of lymph node vascularisation: Resistive index (RI)
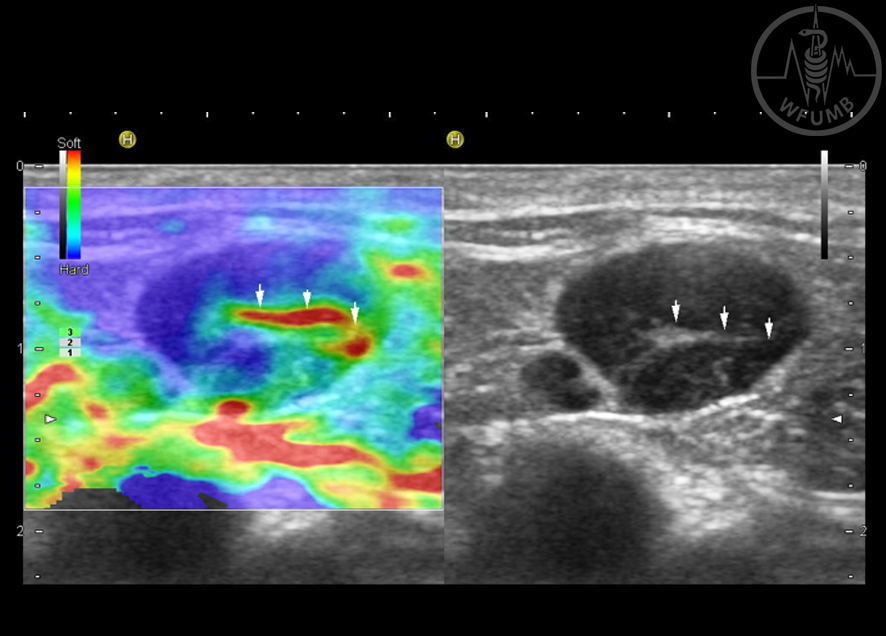
Fig 16.25
Benign and malignant phenotypes of lymph node with strain elastography
Fig 16.26
“Soft hilum” sign with strain elastography; the lymph node hilum is coded red = soft with strain elastography, corresponding to the (compressed) echogenic hilum on B-Mode US
Fig 16.27a
Inflammatory lymph node (peripheral location): swollen, oval (35 x 13 mm, Solbiati index 2.7), well-defined concentric widened hypoechoic cortex with nearly anechoic peripheral areas and compressed echogenic hilum reflex (B-Mode US)
Fig 16.27b
Inflammatory lymph node (peripheral location): increased global vascularity with tree-like branching hilar vessels (CDUS)
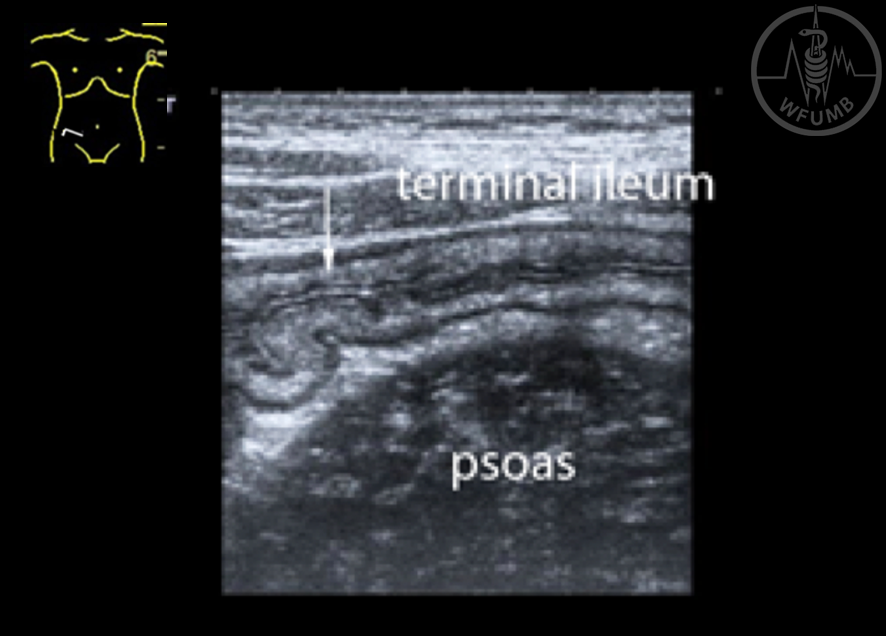
Fig 16.28a
Mesenteric lymphadenitis in a 14 years old boy with right lower quadrant pain. Slightly thickened terminal ileum with preserved layering
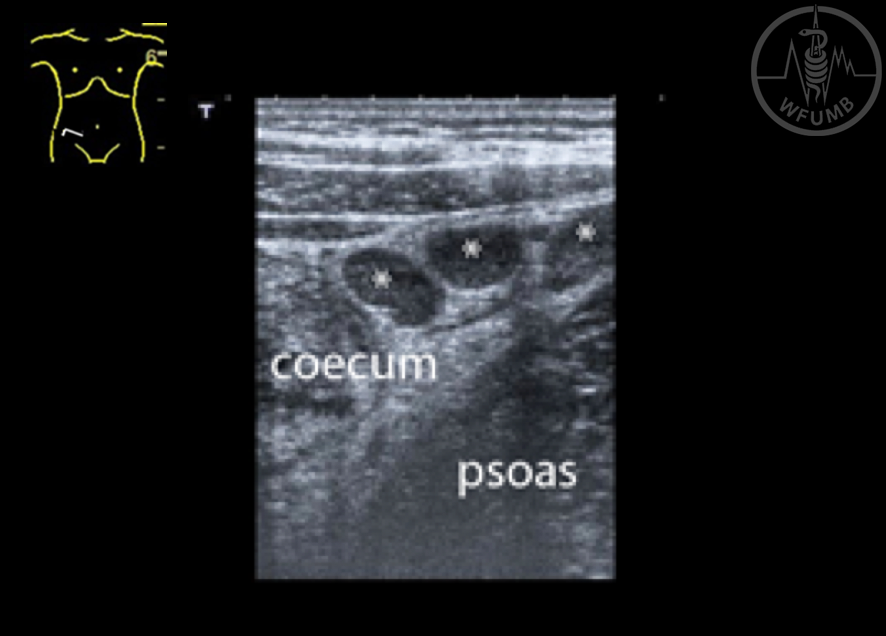
Fig 16.28b
Mesenteric lymphadenitis in a 14 years old boy with right lower quadrant pain. Slightly thickened terminal ileum with preserved layering multiple hypoechoic surrounding lymph nodes (marked with*)
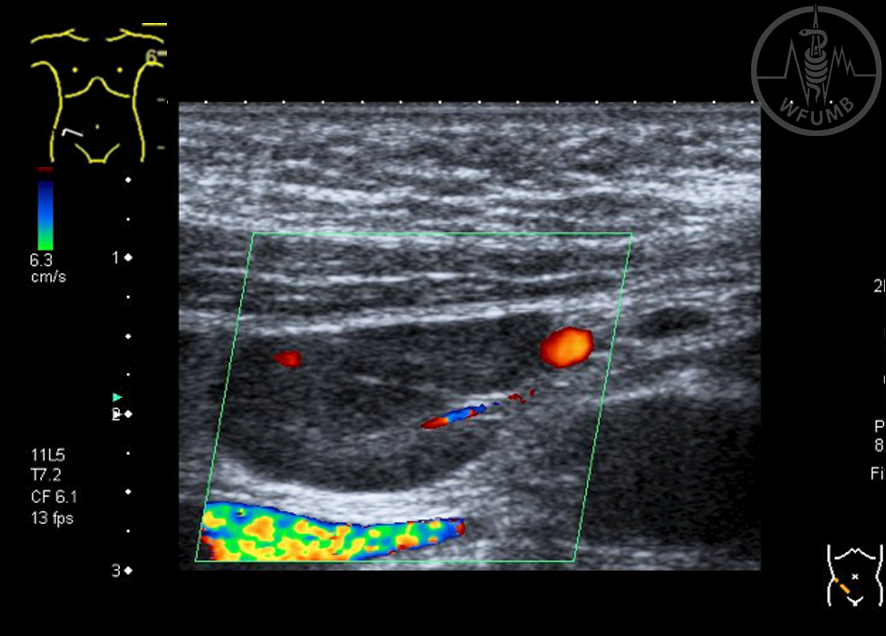
Fig 16.28c
Mesenteric lymphadenitis in a 14 years old boy with right lower quadrant pain. The largest lymph node with compressed echogenic hilum with visible hilar artery (CDUS)
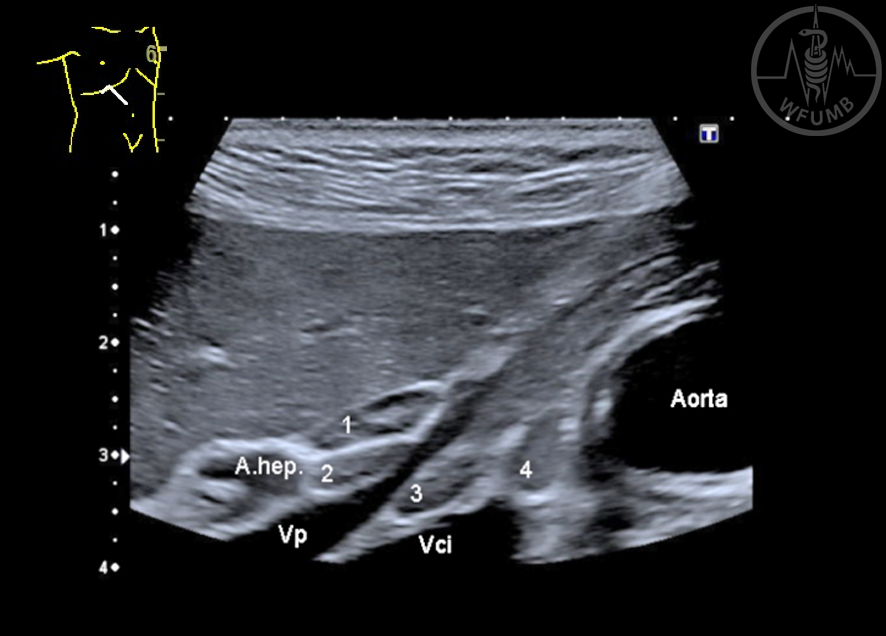
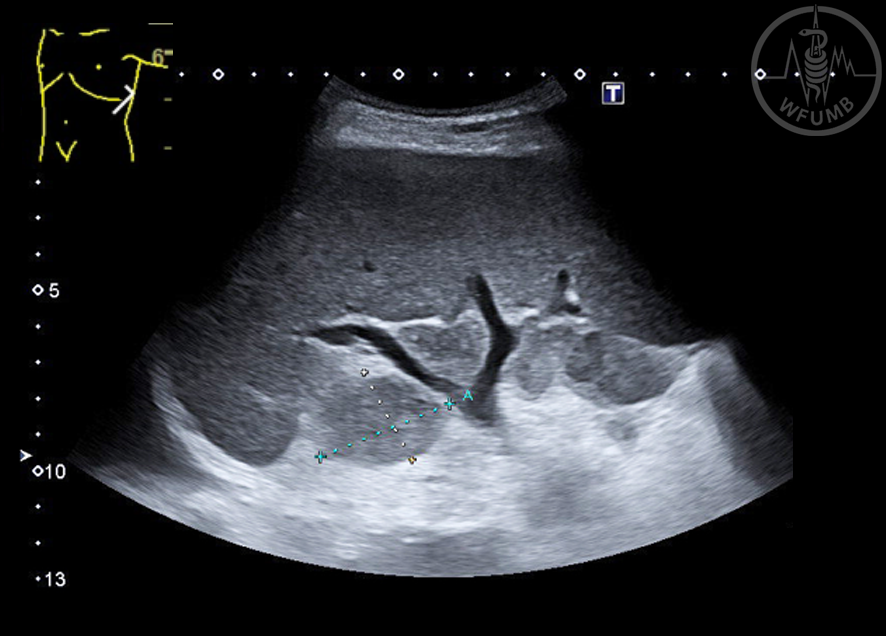
Fig 16.29
Reactive lymph nodes in the liver hilum in a patient with autoimmune hepatitis. 4 enlarged, oval lymph nodes are seen, one with well-defined hypoechoic cortex and echogenic hilum (A.hep: hepatic artery; Vp: portal vein; Vci: inferior caval vein)
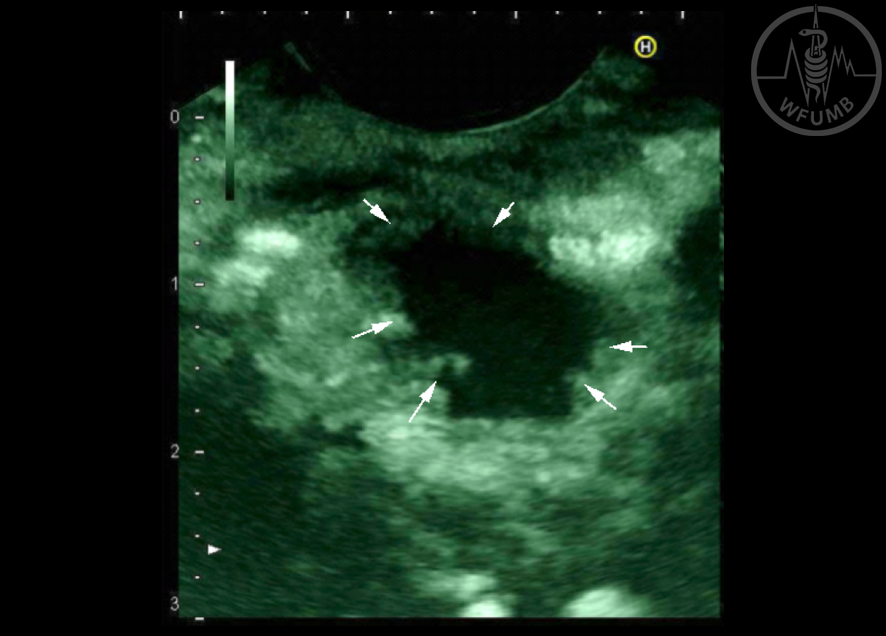
Fig 16.30
Large round hypoechoic lymph node metastasis (48 x 42 mm, Solbiati index 1.14) with a central anechoic area (necrosis) (*) and surrounding edema (arrows) in a patient with pancreatic acinus cell cancer
Fig 16.31a
Cervical lymph node metastases in a patient with malignant melanoma. The lymph nodes are hypoechoic (B mode US)
Fig 16.31b
Cervical lymph node metastases in a patient with malignant melanoma. The lymph nodes are hypoechoic with a predominantly peripheral vascular pattern (CDUS)
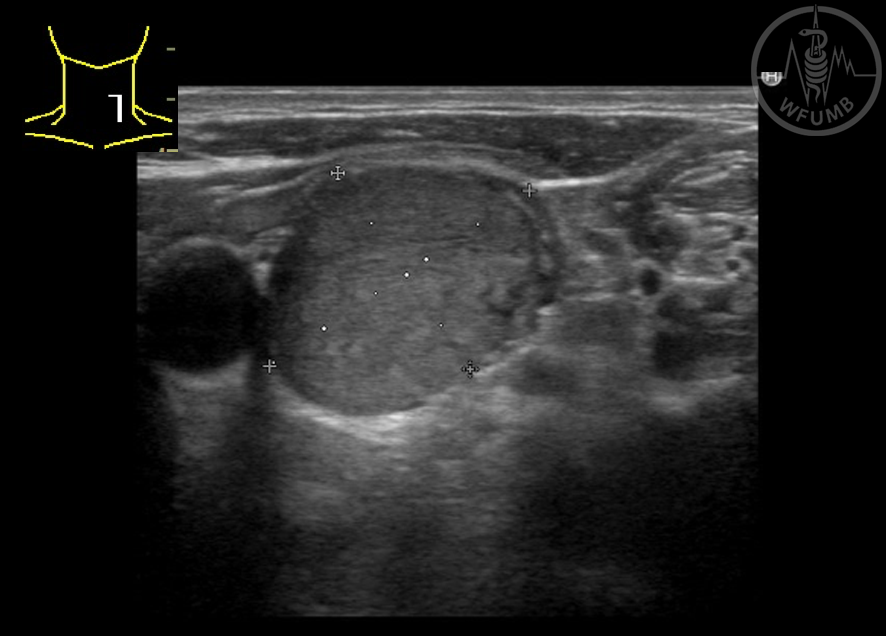
Fig 16.32a
Generalised metastatic lymphadenopathy in a patient with seminoma: well-defined hypoechoic round-oval cervical lymph nodes with loss of echogenic hilum, maximum 14 x 9 mm, Solbiati index 1.56 (B-Mode US)
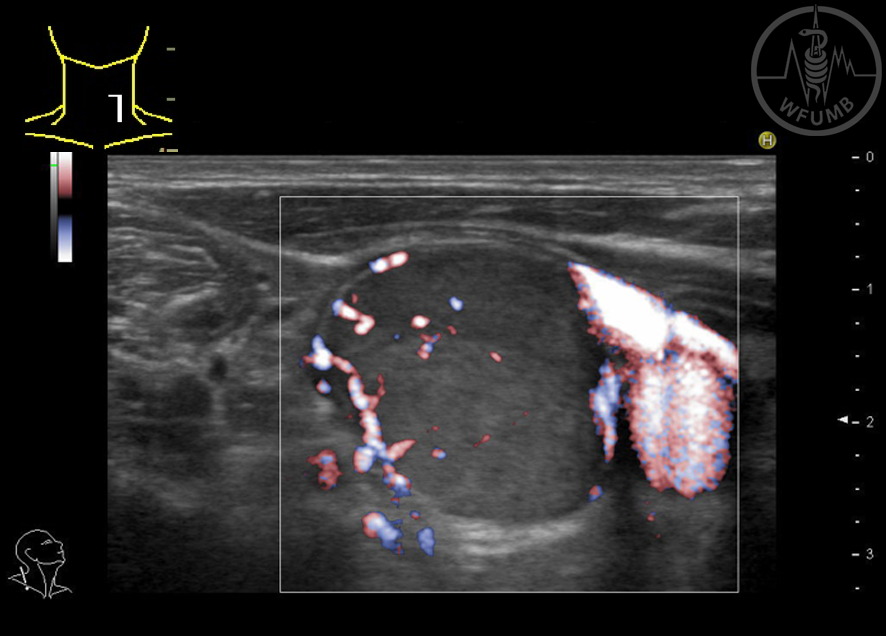
Fig 16.32b
Generalised metastatic lymphadenopathy in a patient with seminoma: well defined large hypoechoic pelvic lymph node (35 x 22 mm, Solbiati index 1,59) with compressed hilum, preserved hilar vessels and additional peripheral neovascularisation (CDUS)
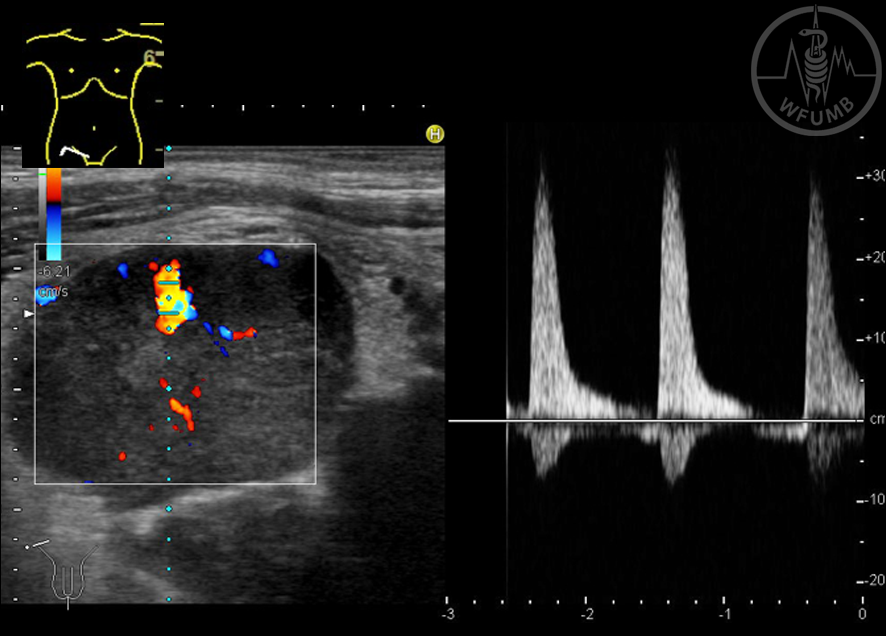
Fig 16.32c
Generalised metastatic lymphadenopathy in a patient with seminoma: large hypoechoic inguinal lymph nodes with aberrant vessels and a very high resistive index of 0.93 in the hilar artery (Peak systolic velocity 30 cm/s, end-diastolic velocity approximately 2 cm/s) (CDUS)
Fig 16.33a
Jugular round lymph node (25 x 19 mm, Solbiati index 1.3) with medium echogenicity and loss of echogenic hilum (B-Mode) in a patient with peripheral non-small cell lung cancer
Fig 16.33b
Jugular round lymph node (25 x 19 mm, Solbiati index 1.3) in a patient with peripheral non-small cell lung cancer. This lymph node has a malignant phenotype on CDUS
Fig 16.33c
Jugular round lymph node (25 x 19 mm, Solbiati index 1.3) in a patient with peripheral non-small cell lung cancer. This lymph node has a malignant phenotype on strain elastography
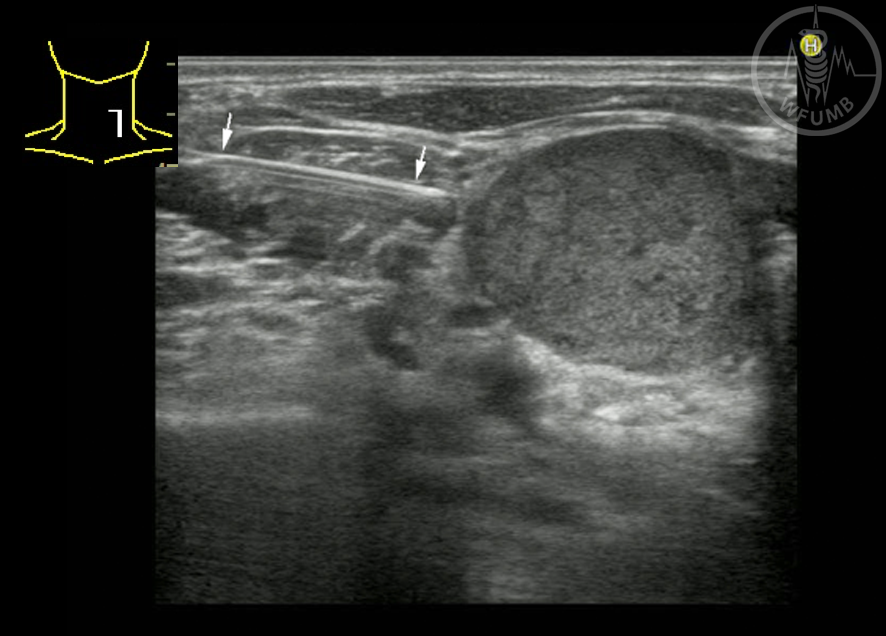
Fig 16.33d
Jugular round lymph node (25 x 19 mm, Solbiati index 1.3) in a patient with peripheral non-small cell lung cancer. Due to the fact that histologic proof of metastasis at this N3 station would result in palliative management of this patient, US-guided biopsy was performed (arrows mark the 18 G, sping-loaded needle)
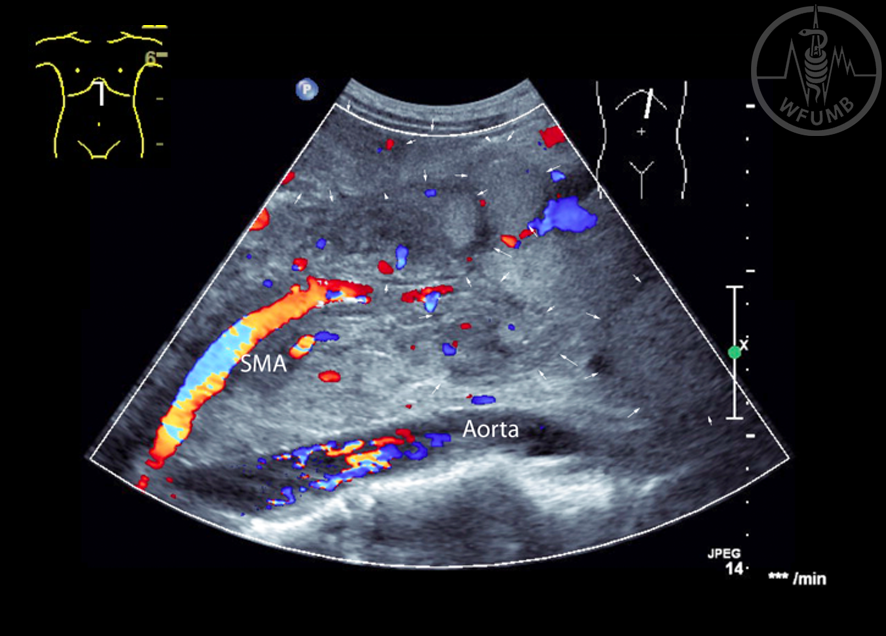
Fig 16.34a
Bulky non-Hodgkin’s lymphoma with large, confluent lymph nodes in front of the aorta, surrounding the superior mesenteric artery (SMA) (B-Mode and CDUS). Arrows mark the ill-defined borders of single large lymphomas forming the bulky lesion)
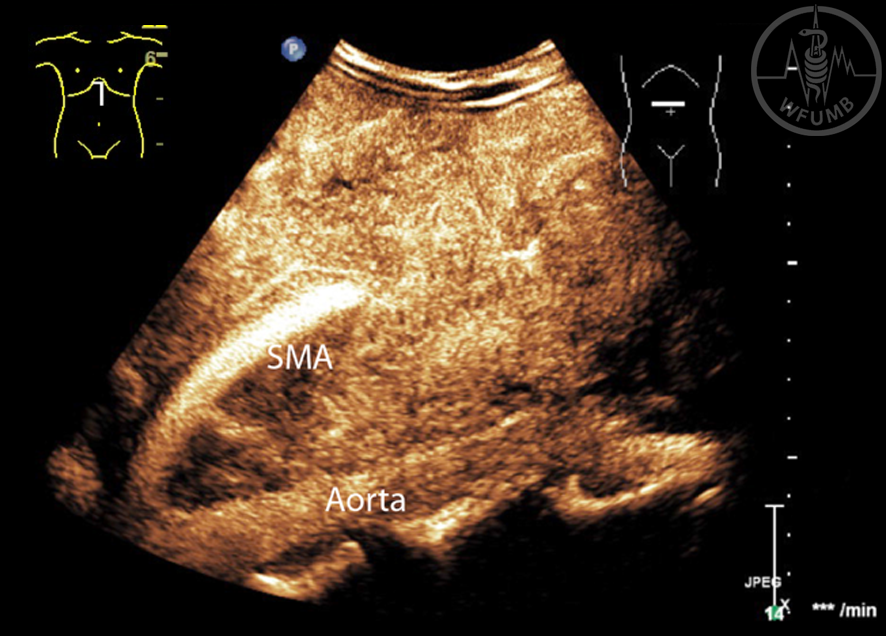
Fig 16.34b
Bulky non-Hodgkin’s lymphoma with large, confluent lymph nodes in front of the aorta, surrounding the superior mesenteric artery (SMA). Contrast-enhanced US shows a rich vascularity of the bulky lesion with fast and intense arterial enhancement
Fig 16.34c
Bulky non-Hodgkin’s lymphoma with large, confluent lymph nodes in front of the aorta, surrounding the superior mesenteric artery (SMA). Contrast-enhanced US shows a rich vascularity of the bulky lesion with fast and intense arterial enhancement
Fig 16.35
Splenomegaly and enlarged hilar lymph nodes in a patient with chronic lymphocytic leukaemia
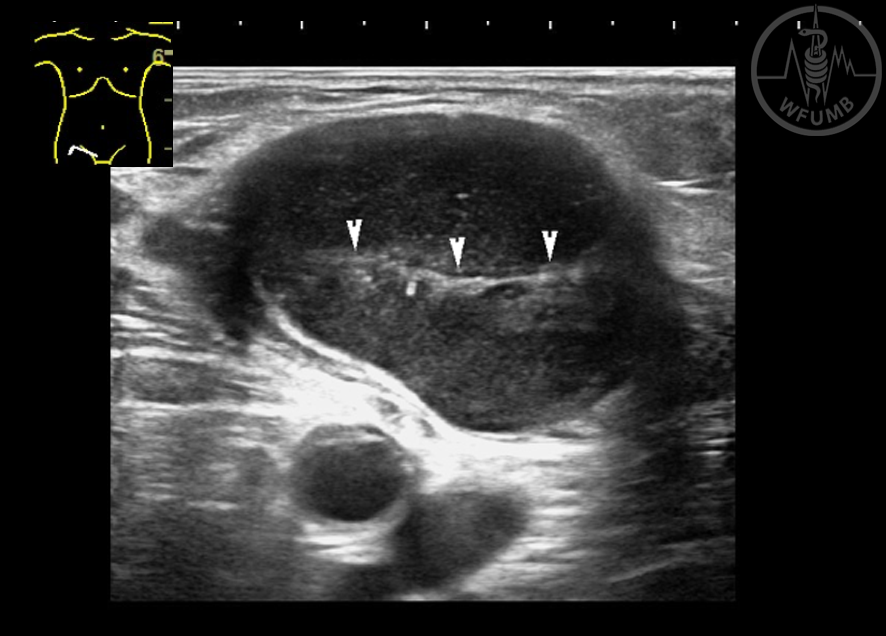
Fig 16.36
Typical B-Mode appearance of malignant lymphoma (inguinal location): hypoechoic round-oval lymph node with hypoechoic reticular echo-pattern and compressed echogenic hilum (arrow-heads)