Alina Constantin1, Cătălin Copăescu2, Victor Tomulescu2, Adrian Săftoiu3
1Gastroenterology Department, Ponderas Academic Hospital Bucharest
2Surgical Department, Ponderas Academic Hospital Bucharest
3Research Center of Gastroenterology and Hepatology, University of Medicine and Pharmacy Craiova, Romania
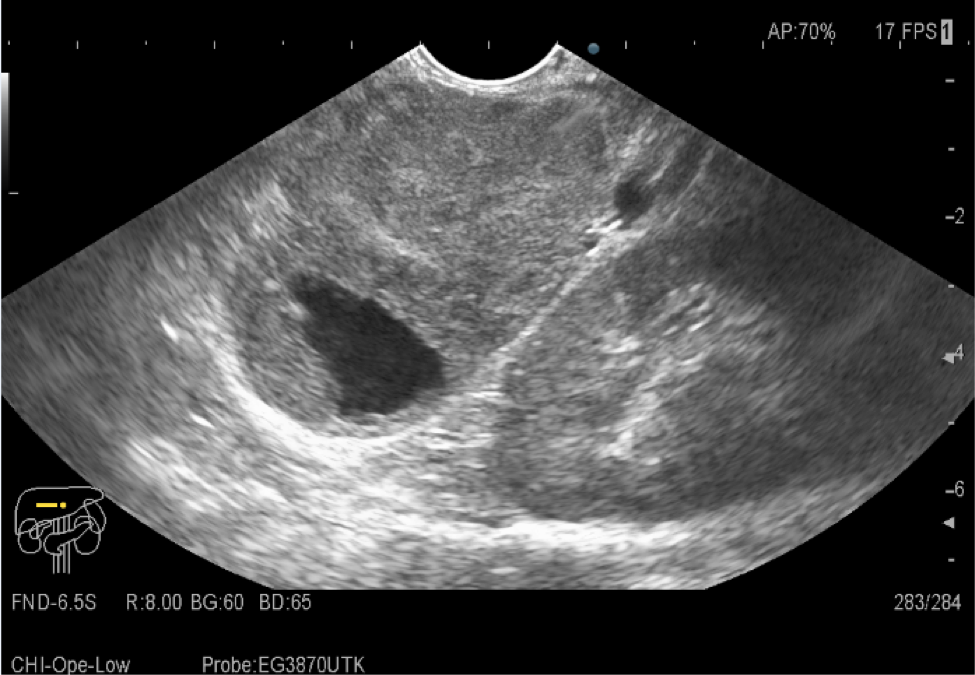
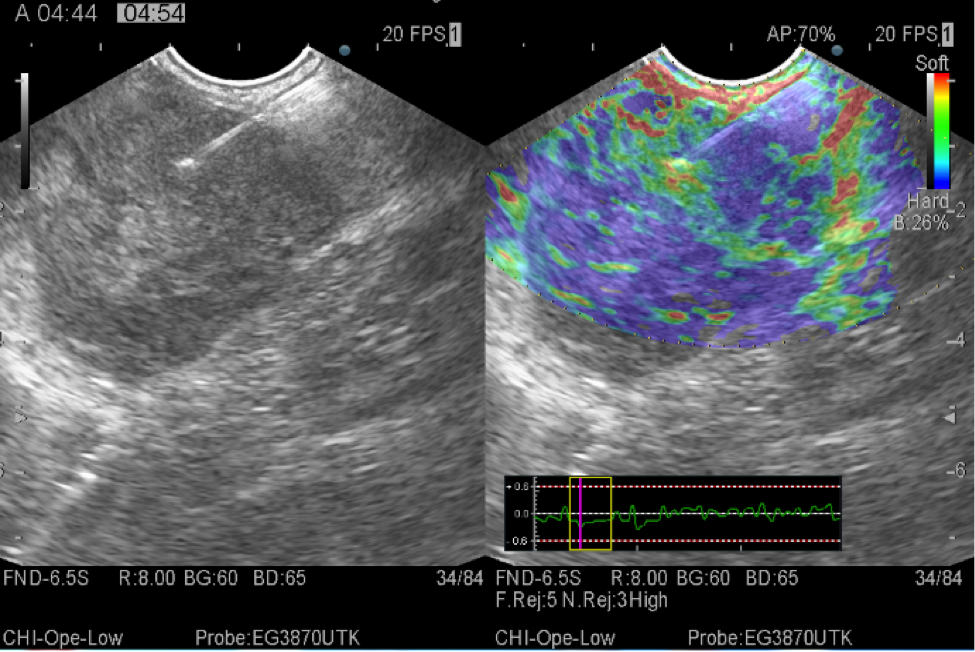
SPN which occurs in young women in the third decade of life has well-defined borders and variable central areas with cystic degeneration, necrosis, or hemorrhage (Figure 1a). Contrast enhanced EUS reveals in SPN hypoenhancement in the the arterial and venous phase (Video 1). In contrast, NETs are hyperenhancing lesions. Elastography shows stiffer tissue compared to the surrounding (Figure 1b). Biopsy and immunohistochemical staining were performed for final diagnosis.
Neuroendocrine tumor (NET) and solid-pseudopapillary neoplasm (SPN) are two types of pancreatic tumor that were sometimes difficult to differentiate. Biopsy and immunohistochemical analysis obtained by a histological needle biopsy plays a crucial role in differentiating these two tumor types, E-cadherin, chromogranin A, and β-catenin representing the most useful markers which should be employed for differentiating between NET and SPN.
Yusuke Ohara, Tatsuya Oda, Shinji Hashimoto. Pancreatic neuroendocrine tumor and solid-pseudopapillary neoplasm: Key immunohistochemical profiles for differential diagnosis, World J Gastroenterol 2016;22(38):8596-8604.