
Webinar: WFUMB ‘Ultrasound, the Best’ Cases
July 7, 2020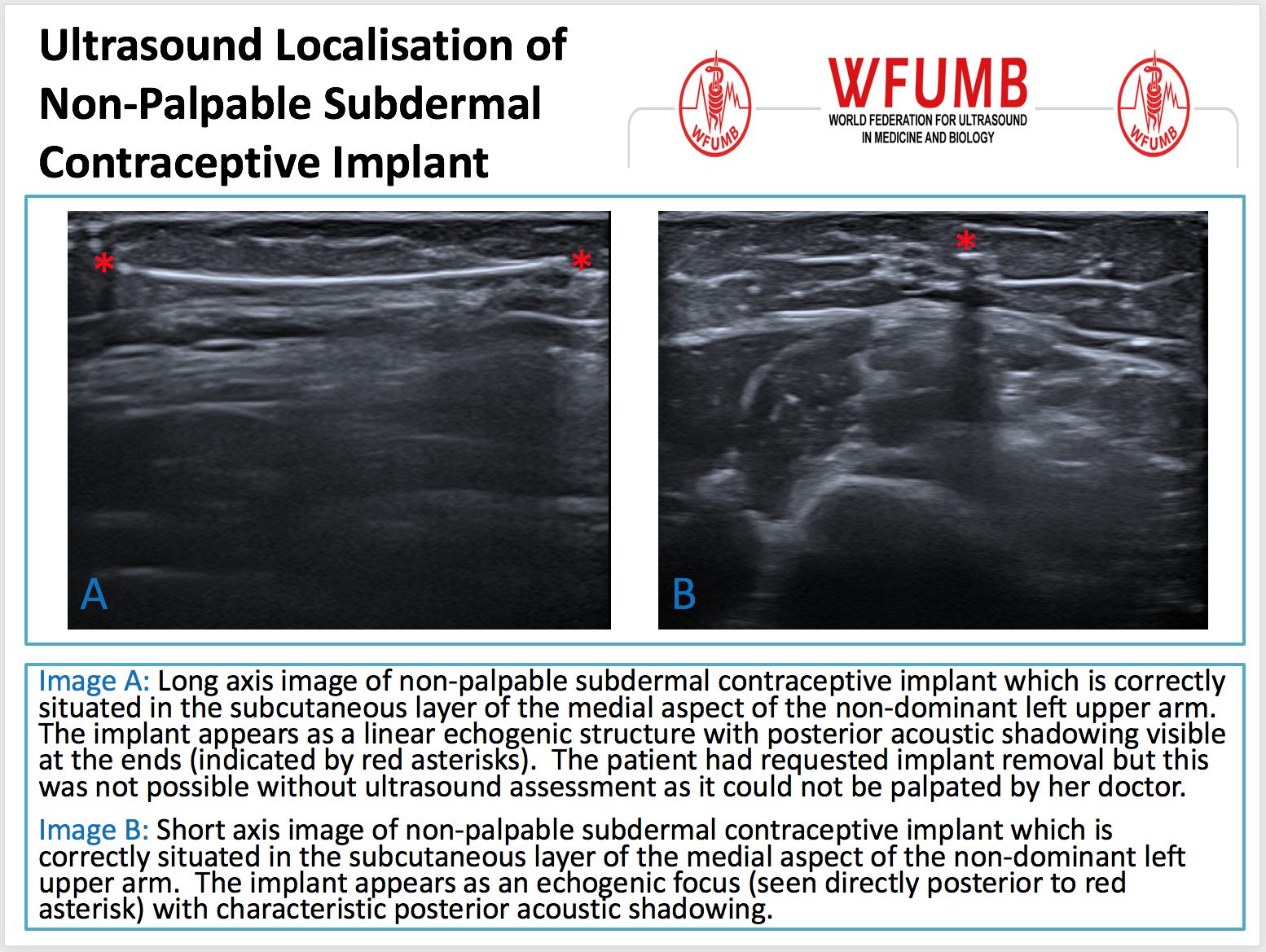
Ultrasound the Best #04: Ultrasound Localisation of Non-Palpable Subdermal Contraceptive Implant
July 22, 2020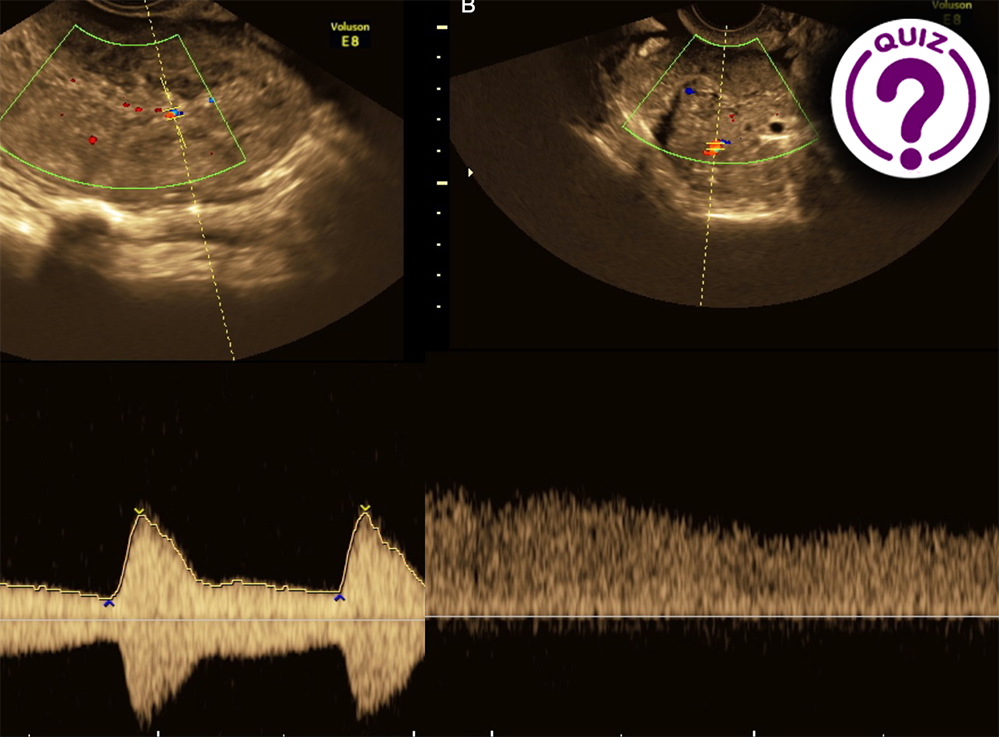
A female with an acute onset of severe pain in the lower abdomen
Dr. Serghei Puiu, Dr, PhD
Department of Radiology and Imaging, State University of Medicine and Pharmacy “Nicoale Testemitanu”, Chisinau, Republic of Moldova
Corresponding author: Serghei Puiu
Email: puiusv@yahoo.com
Clinical History:
A 47-year-old lady was referred to our department for a second opinion before surgery regarding an ovarian mass suspect of an ovarian tumour. She had an acute onset of severe pain in the lower right abdominal quadrant one week previously, which disappeared spontaneously. When she presented in our department, she had no pain or fever. Blood tests, including tumour markers, were normal.
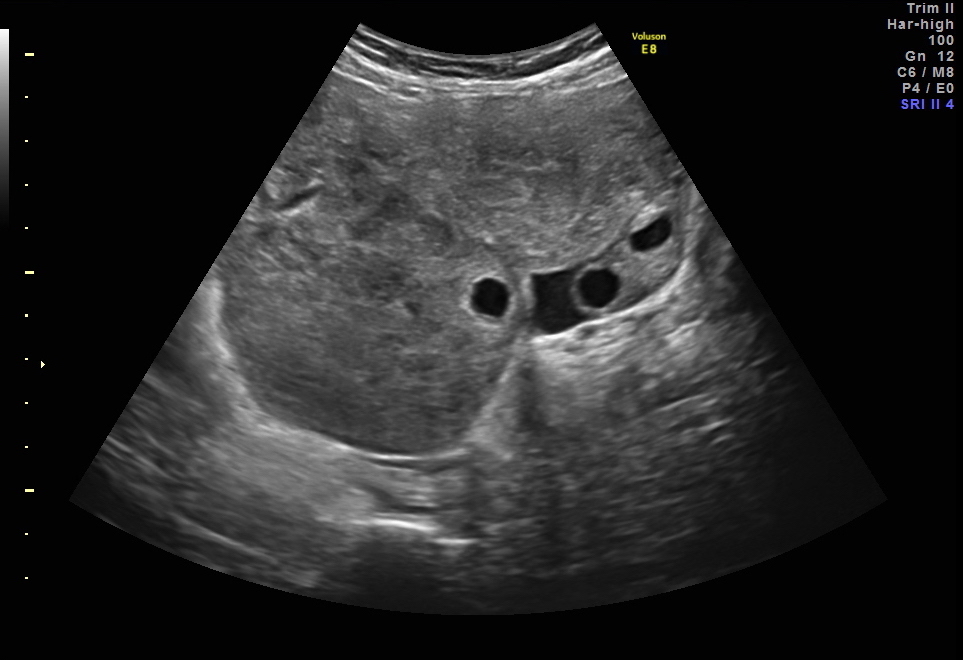
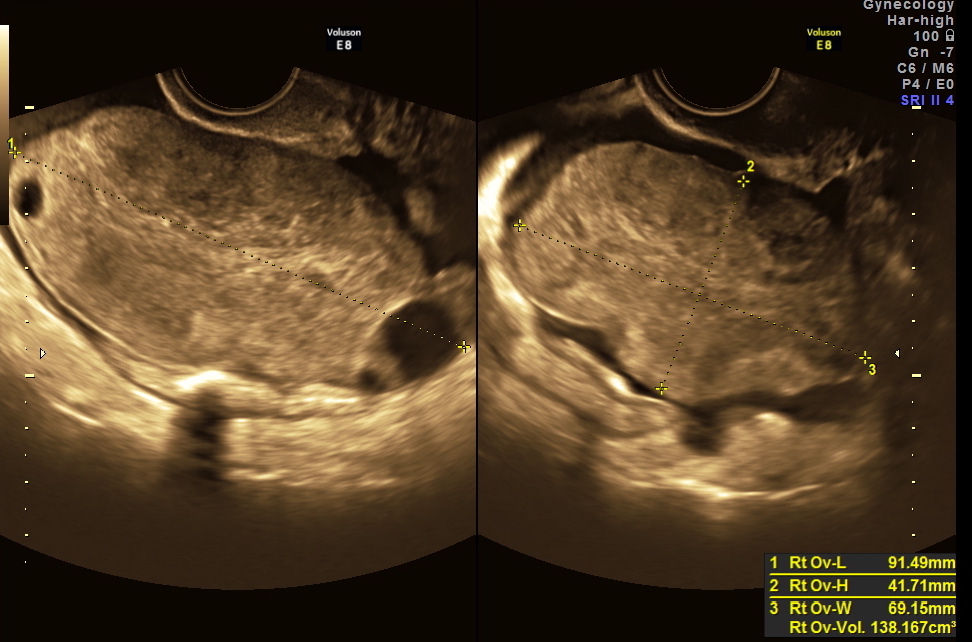
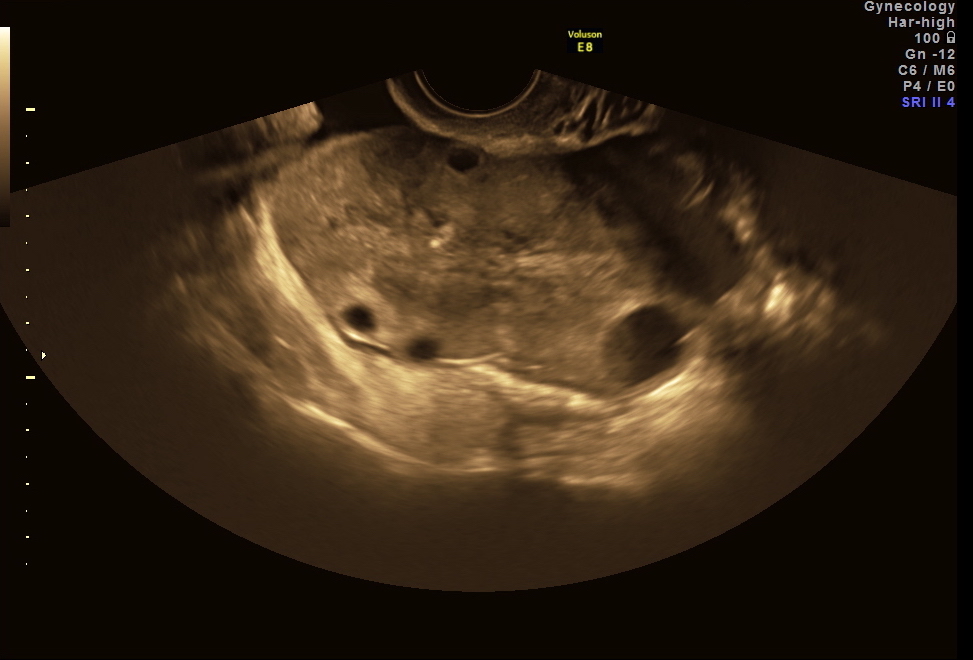
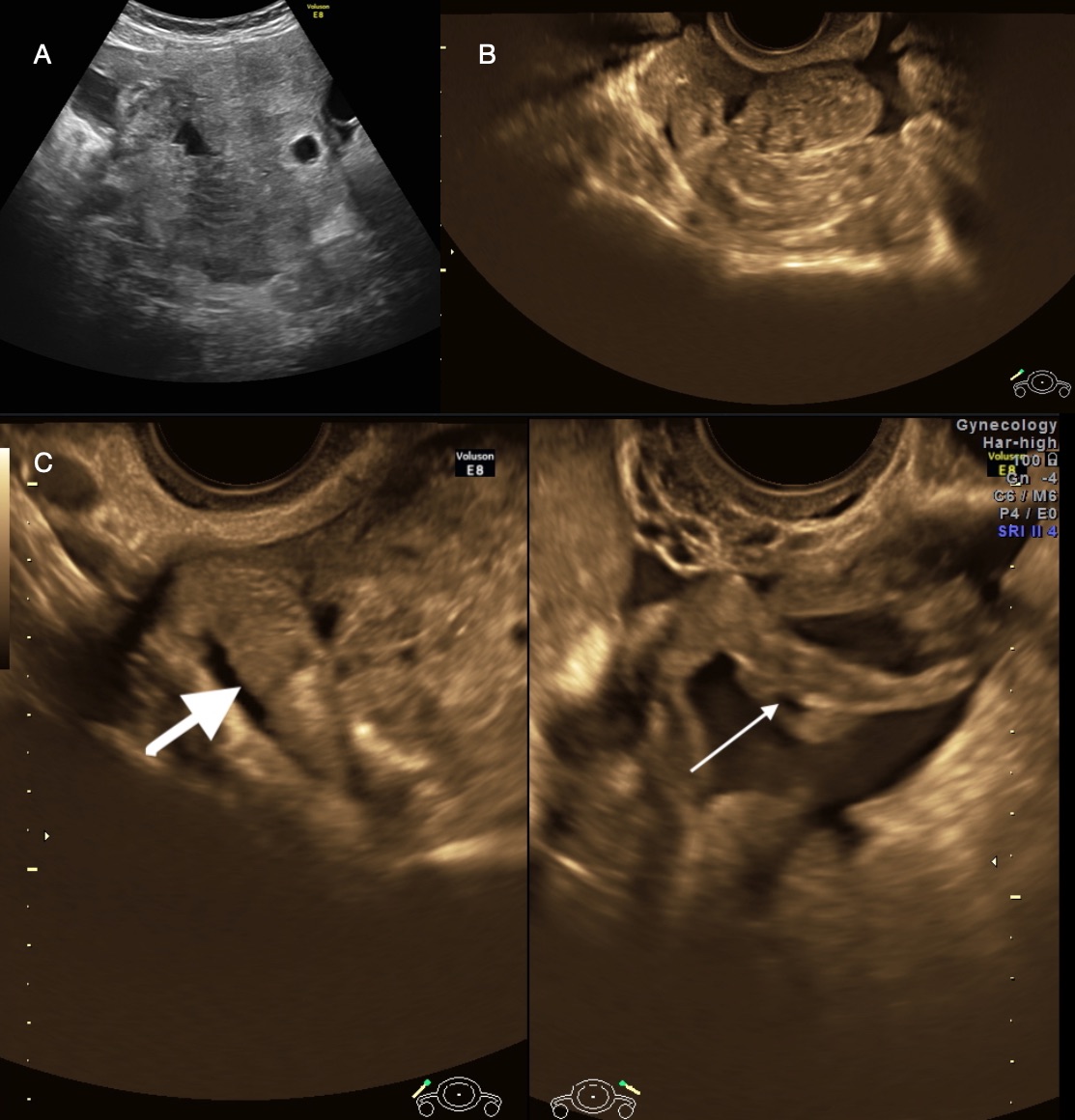
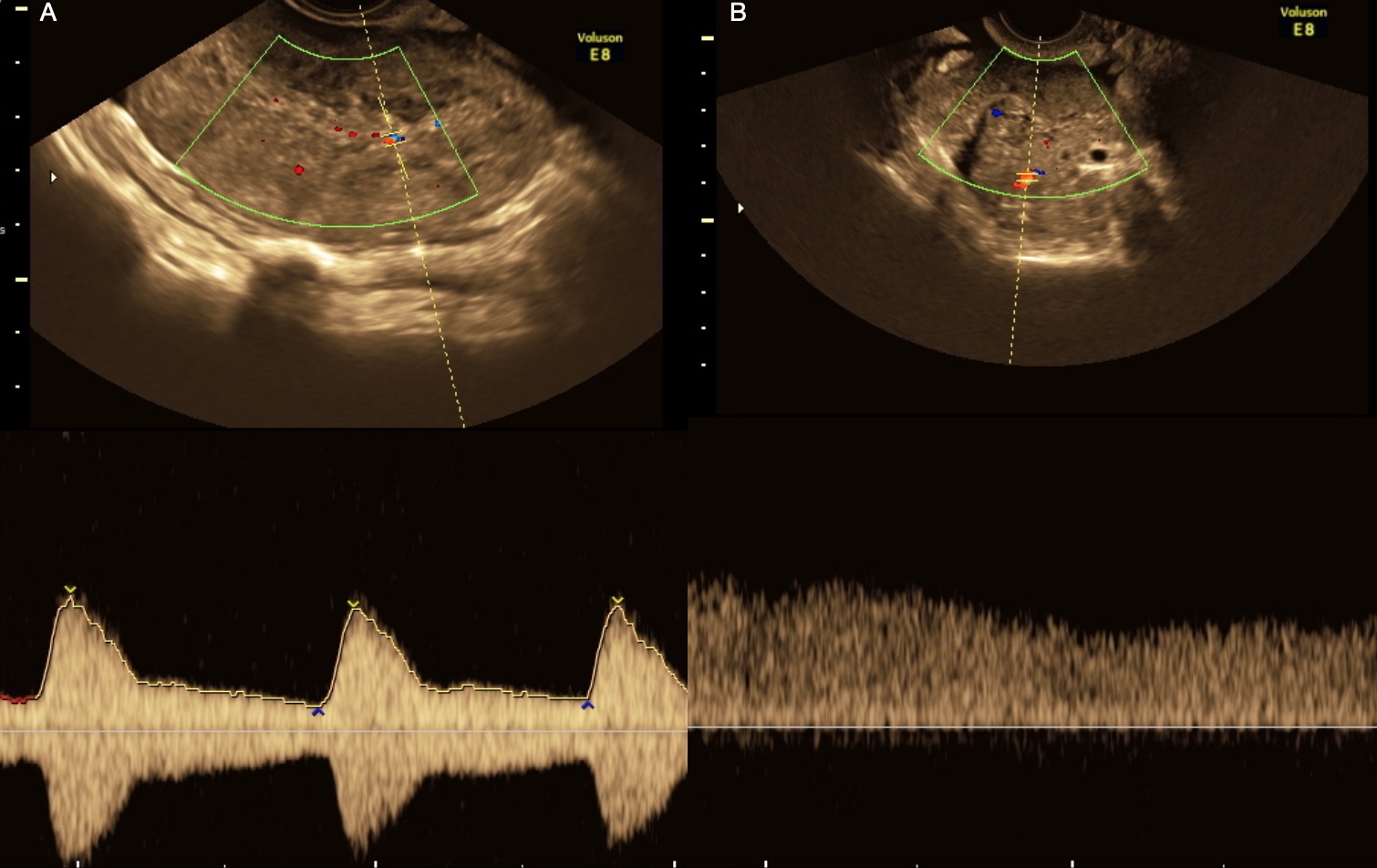
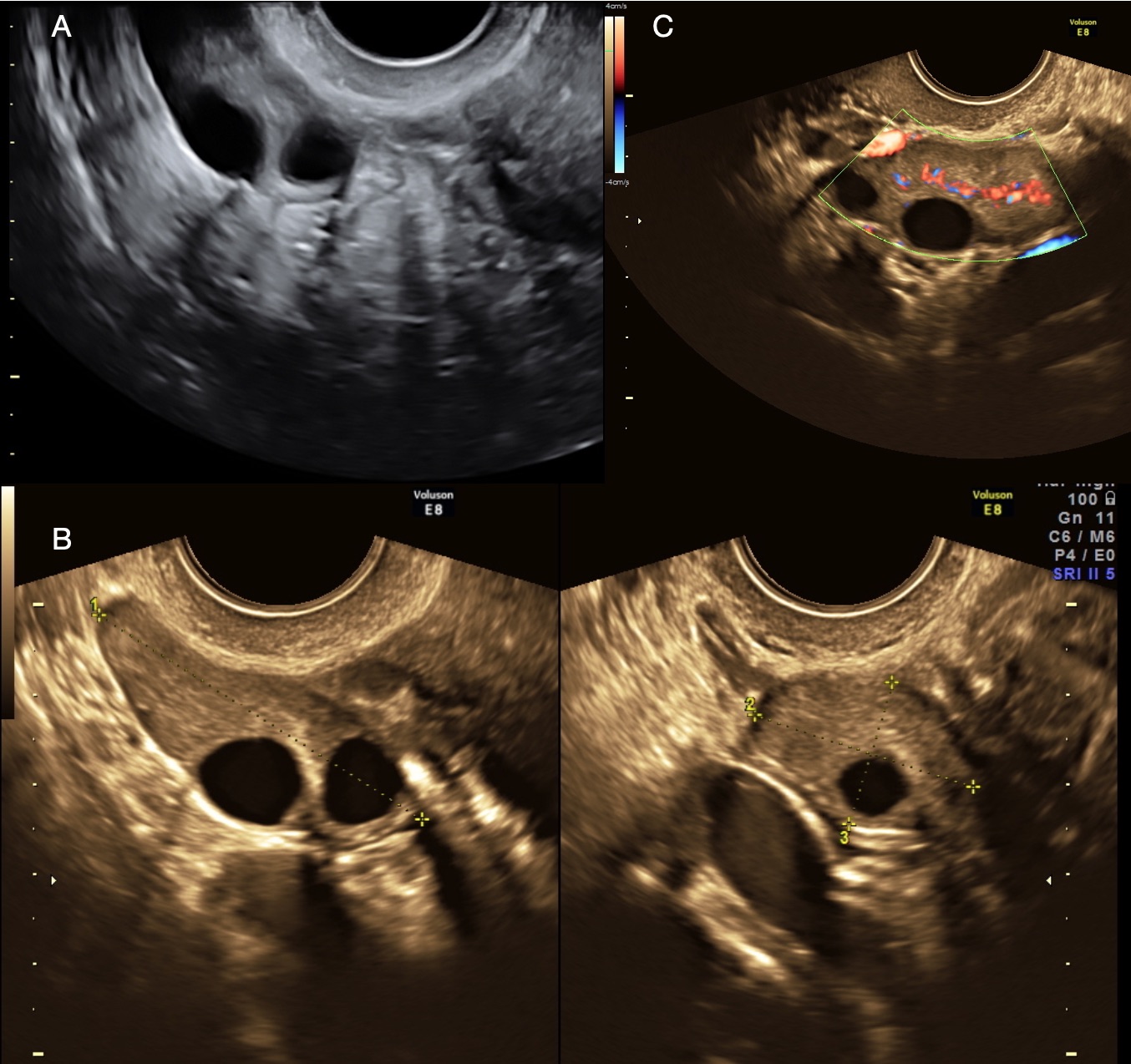
Transabdominal and transvaginal ultrasound scans were performed. They showed an enlarged, but well-defined right ovary, appearing as a mass (Fig. 1-2). The stroma was heterogeneous due to edema displacing the follicles peripherally (Fig. 3). An echogenic thickened fallopian tube seemed to wrap the enlarged ovary (Fig. 4 a-c). The ovarian arterial and venous flow was preserved (Fig. 5 a-b). A small fluid collection in the Douglas pouch and around the ovary was seen. There was a slight pain on transducer touch.
Quiz-summary
0 of 1 questions completed
Questions:
- 1
Information
View the July Case below, answer the question and then click check >
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 1 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
- 1
- Answered
- Review
-
Question 1 of 1
1. Question
Question: What is the most likely diagnose based on the above findings?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer is:
Spontaneous complete detorsion of previously twisted ovary/adnexa
Explanation:
We have shown a case of spontaneous detorsion of a previously twisted ovary. Ovarian or adnexal (ovary and fallopian tube) torsion is a surgical emergency that requires prompt diagnosis and treatment. It is defined as complete or partial rotation of the adnexa around the pedicle, causing lymphatic and venous ovarian congestion, followed by ischemia and necrosis due to arterial occlusion when untreated. It can rapidly progress to a stage of hemorrhagic necrosis in a few hours or remain at the stage of edema for several days, rarely resulting in complete spontaneous detorsion.
Adnexal torsion accounts for approximately 3% of all gynecological emergencies [1]. The torsion may involve normal adnexa, however ovarian enlargement predisposes to torsion, commonly by corpus luteal cyst, benign ovarian tumour or ovulation induction [2, 3]. Prompt diagnosis is important to prevent irreversible damage of the ovary. However, the diagnosis can be challenging because clinical presentation of ovarian torsion is variable and often misleading. Definitive diagnosis is often achieved by surgery [4, 5]. Sonography is usually the first imaging tool used for evaluation, but the diagnostic accuracy is rather poor (46-74%) [6-9]. The sonographic findings vary from the enlarged ovary simulating a mass with peripherally displaced follicles in the early phase and a “solid” avascular appearance of the ovary in the late phase. However, Doppler is not a very sensitive for diagnosing ovarian torsion, and normal flow does not rule out torsion [10, 11]. An important sonographic sign of adnexal torsion is the “whirlpool sign”. A coiling pattern of ovarian vessels in the ovarian ligament refers to the sonographic appearance of the twisted ovarian vascular pedicle and has been shown to have up to 87% diagnostic accuracy for ovarian torsion [12-14]. In the rare cases of spontaneous complete detorsion the ultrasound findings can persist for a while after the untwisting because the edema does not disappear immediately [15].
In conclusion, the diagnosis of ovarian torsion remains challenging. In a patient who presents with acute pain and an ovary that demonstrates sonographic findings consistent with ovarian torsion, the diagnosis should be suggested even in the presence of documented arterial blood flow.
References
- Rochelle F. Andreotti, Sara M. Harvey. Sonographic Evaluation of Acute Pelvic Pain. J Ultrasound Med 2012; 31:1713–1718.
- Mashiach S, Bider D, Moran O, Goldenberg M, Ben-Rafael Z. Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy. Arch Gynecol Obstet 2002;267(1):4 –6.
- Purcell K, Wheeler JE. Benign disorders of the ovaries and oviducts. In: De Cerney A, Nathan L, editors. Current obstetric and gynecologic diagnosis and treatment. New York: McGraw-Hill; 2003.
- Kokoska ER, Keller MS, Weber TR. Acute ovarian torsion in children. Am J Surg 2000; 180: 462–465.
- Gordon JD, Hopkins KL, Brooke JR, Giudice LC. Adnexal torsion: color Doppler diagnosis and laparoscopic treatment. Fertil Steril 1994; 61: 383–385.
- Mazouni C, Bretelle F, Ménard JP, Blanc B, Gamerre M. Diagnosis of adnexal torsion and predictive factors of adnexal necrosis. Gynecol Obstet Fertil 2005; 33:102–106.
- Bar-On S, Mashiach R, Stockheim D, et al. Emergency laparoscopy for suspected ovarian torsion: are we too hasty to operate? Fertil Steril 2010; 93:2012–2015.
- Reuven Mashiach, Nir Melamed, Noa Gilad, Gadi Ben-Shitrit, Israel Meizner. Sonographic Diagnosis of Ovarian Torsion. Accuracy and Predictive Factors. J Ultrasound Med 2011; 30: 1205–1210.
- Cohen SB, Weisz B, Seidman DS, Mashiach S, Lidor AL, Goldenberg M. Accuracy of the preoperative diagnosis in 100 emergency laparoscopies performed due to acute abdomen in nonpregnant women. J Am Assoc Gynecol Laparosc 2001; 8: 92–94.
- Hurh PJ, Meyer JS, Shaaban A. Ultrasound of a torsed ovary: characteristic gray-scale appearance despite normal arterial and venous flow on Doppler. Pediatr Radiol 2002; 32(8): 586- 8.
- Shadinger LL, Andreotti RF, Kurian RL. Preoperative sonographic and clinical characteristics as predictors of ovarian torsion. J Ultrasound Med 2008; 27:7–13.
- Lee EJ, Kwon HC, Joo HJ, Suh JH, Fleischer AC. Diagnosis of ovarian torsion with color Doppler sonography: depiction of twisted vascular pedicle. J Ultrasound Med 1998; 17:83–89.
- Vijayaraghavan SB. Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med 2004; 23: 1643–1649.
- V. Valsky, E. Esh-Broder, S.M. Cohen, M. Lipschuetz and S. Yagel. Added value of the gray-scale whirlpool sign in the diagnosis of adnexal torsion. Ultrasound Obstet Gynecol 2010; 36: 630–634.
- Ghossain MA, Hachem K, Aoun NJ, Haddad-Zebouni S, Mansour F, Suidan JS, Abboud J (2006) Spontaneous detorsion of the ovary: can it be diagnosed by MRI? J Magn Reson Imaging 24(4):880–885.
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer is:
Spontaneous complete detorsion of previously twisted ovary/adnexa
Explanation:
We have shown a case of spontaneous detorsion of a previously twisted ovary. Ovarian or adnexal (ovary and fallopian tube) torsion is a surgical emergency that requires prompt diagnosis and treatment. It is defined as complete or partial rotation of the adnexa around the pedicle, causing lymphatic and venous ovarian congestion, followed by ischemia and necrosis due to arterial occlusion when untreated. It can rapidly progress to a stage of hemorrhagic necrosis in a few hours or remain at the stage of edema for several days, rarely resulting in complete spontaneous detorsion.
Adnexal torsion accounts for approximately 3% of all gynecological emergencies [1]. The torsion may involve normal adnexa, however ovarian enlargement predisposes to torsion, commonly by corpus luteal cyst, benign ovarian tumour or ovulation induction [2, 3]. Prompt diagnosis is important to prevent irreversible damage of the ovary. However, the diagnosis can be challenging because clinical presentation of ovarian torsion is variable and often misleading. Definitive diagnosis is often achieved by surgery [4, 5]. Sonography is usually the first imaging tool used for evaluation, but the diagnostic accuracy is rather poor (46-74%) [6-9]. The sonographic findings vary from the enlarged ovary simulating a mass with peripherally displaced follicles in the early phase and a “solid” avascular appearance of the ovary in the late phase. However, Doppler is not a very sensitive for diagnosing ovarian torsion, and normal flow does not rule out torsion [10, 11]. An important sonographic sign of adnexal torsion is the “whirlpool sign”. A coiling pattern of ovarian vessels in the ovarian ligament refers to the sonographic appearance of the twisted ovarian vascular pedicle and has been shown to have up to 87% diagnostic accuracy for ovarian torsion [12-14]. In the rare cases of spontaneous complete detorsion the ultrasound findings can persist for a while after the untwisting because the edema does not disappear immediately [15].
In conclusion, the diagnosis of ovarian torsion remains challenging. In a patient who presents with acute pain and an ovary that demonstrates sonographic findings consistent with ovarian torsion, the diagnosis should be suggested even in the presence of documented arterial blood flow.
References
- Rochelle F. Andreotti, Sara M. Harvey. Sonographic Evaluation of Acute Pelvic Pain. J Ultrasound Med 2012; 31:1713–1718.
- Mashiach S, Bider D, Moran O, Goldenberg M, Ben-Rafael Z. Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy. Arch Gynecol Obstet 2002;267(1):4 –6.
- Purcell K, Wheeler JE. Benign disorders of the ovaries and oviducts. In: De Cerney A, Nathan L, editors. Current obstetric and gynecologic diagnosis and treatment. New York: McGraw-Hill; 2003.
- Kokoska ER, Keller MS, Weber TR. Acute ovarian torsion in children. Am J Surg 2000; 180: 462–465.
- Gordon JD, Hopkins KL, Brooke JR, Giudice LC. Adnexal torsion: color Doppler diagnosis and laparoscopic treatment. Fertil Steril 1994; 61: 383–385.
- Mazouni C, Bretelle F, Ménard JP, Blanc B, Gamerre M. Diagnosis of adnexal torsion and predictive factors of adnexal necrosis. Gynecol Obstet Fertil 2005; 33:102–106.
- Bar-On S, Mashiach R, Stockheim D, et al. Emergency laparoscopy for suspected ovarian torsion: are we too hasty to operate? Fertil Steril 2010; 93:2012–2015.
- Reuven Mashiach, Nir Melamed, Noa Gilad, Gadi Ben-Shitrit, Israel Meizner. Sonographic Diagnosis of Ovarian Torsion. Accuracy and Predictive Factors. J Ultrasound Med 2011; 30: 1205–1210.
- Cohen SB, Weisz B, Seidman DS, Mashiach S, Lidor AL, Goldenberg M. Accuracy of the preoperative diagnosis in 100 emergency laparoscopies performed due to acute abdomen in nonpregnant women. J Am Assoc Gynecol Laparosc 2001; 8: 92–94.
- Hurh PJ, Meyer JS, Shaaban A. Ultrasound of a torsed ovary: characteristic gray-scale appearance despite normal arterial and venous flow on Doppler. Pediatr Radiol 2002; 32(8): 586- 8.
- Shadinger LL, Andreotti RF, Kurian RL. Preoperative sonographic and clinical characteristics as predictors of ovarian torsion. J Ultrasound Med 2008; 27:7–13.
- Lee EJ, Kwon HC, Joo HJ, Suh JH, Fleischer AC. Diagnosis of ovarian torsion with color Doppler sonography: depiction of twisted vascular pedicle. J Ultrasound Med 1998; 17:83–89.
- Vijayaraghavan SB. Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med 2004; 23: 1643–1649.
- V. Valsky, E. Esh-Broder, S.M. Cohen, M. Lipschuetz and S. Yagel. Added value of the gray-scale whirlpool sign in the diagnosis of adnexal torsion. Ultrasound Obstet Gynecol 2010; 36: 630–634.
- Ghossain MA, Hachem K, Aoun NJ, Haddad-Zebouni S, Mansour F, Suidan JS, Abboud J (2006) Spontaneous detorsion of the ovary: can it be diagnosed by MRI? J Magn Reson Imaging 24(4):880–885.