

Case of the month December 2024: Importance of an incidental finding
December 2, 2024
Case of the month February 2025: Acute leg pain in a sedentary man
February 3, 2025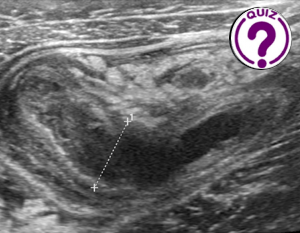
Bahareh Abdolalizadeh 1*, Samir Jawad 1
1 Department of Radiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark; bahareh.abdolalizadeh.01@regionh.dk
* Correspondence: bahareh.abdolalizadeh.01@regionh.dk
Clinical history
An 11-year-old girl presented to the emergency department with a 2-day history of right lower quadrant (RLQ) abdominal pain, loss of appetite and a low-grade fever of approximately 38°C. She denied other symptoms such as nausea, vomiting, or diarrhea. On physical examination, there was localized tenderness in the RLQ with no signs of rebound tenderness. An ultrasound examination was requested.
Images
Quiz-summary
0 of 4 questions completed
Questions:
- 1
- 2
- 3
- 4
Information
View the January Case below, answer the question and then click check >
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 4 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- Answered
- Review
-
Question 1 of 4
1. Question
Question 1: Based on the clinical presentation and initial ultrasound findings, what is the most likely diagnosis?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q1 is: Acute appendicitis
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q1 is: Acute appendicitis
-
Question 2 of 4
2. Question
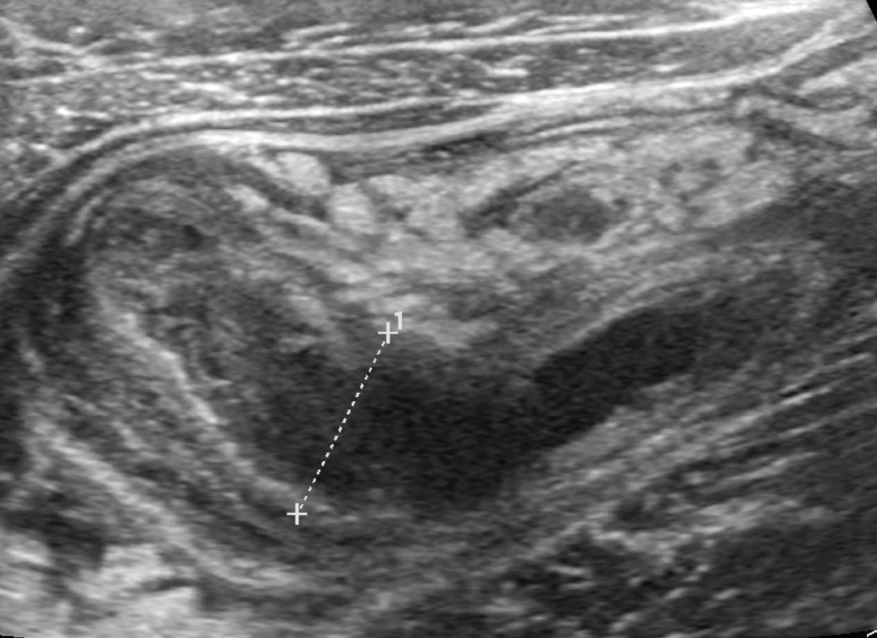
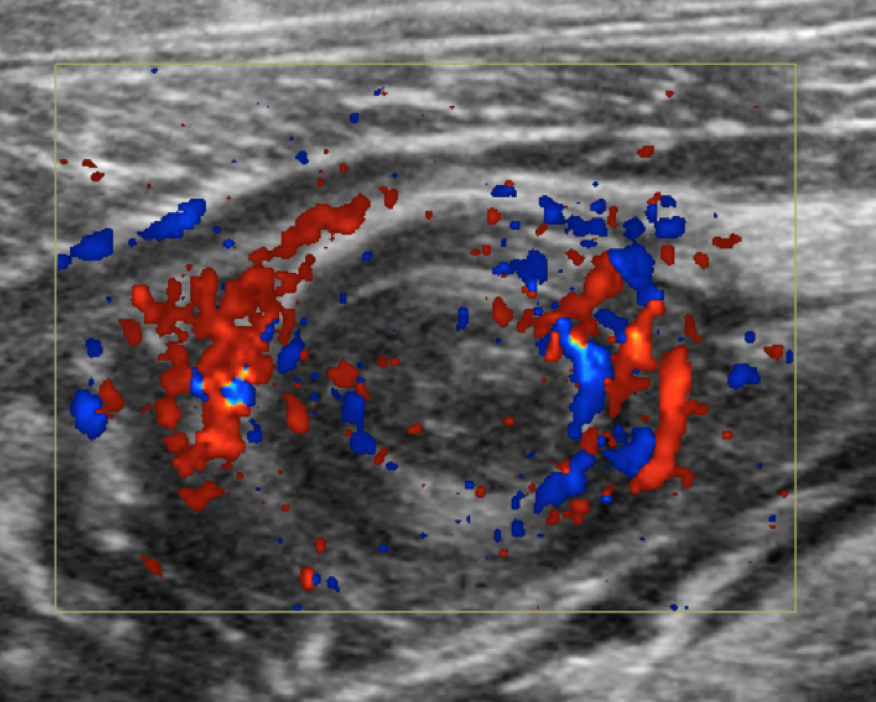
The first ultrasound image shows a blind-ending, sausage-like structure with alternating hyperechoic and hypoechoic layers, including an outermost hypoechoic layer. The fluid-distended lumen measures 12 mm in diameter consistent with appendicitis. On color Doppler there is increased blood flow (hyperemia) in the appendiceal wall.
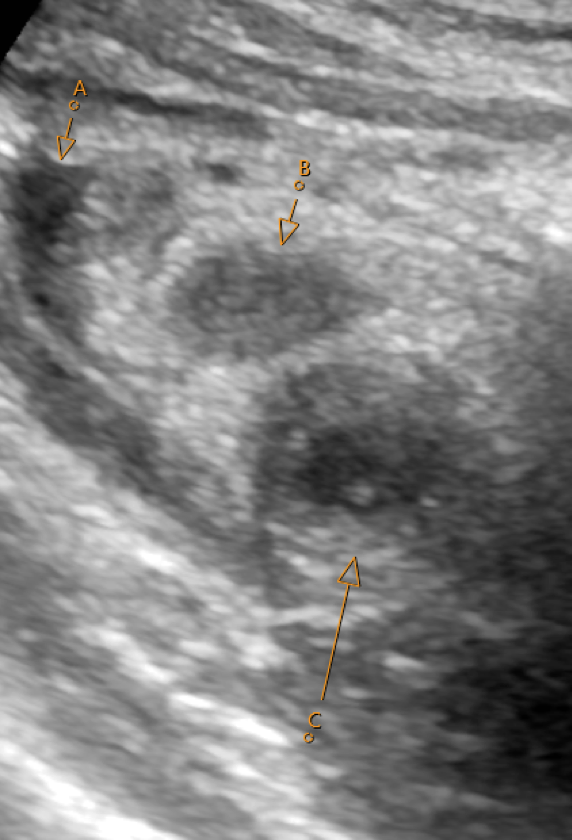
Image 3: Transverse ultrasound image RLQQuestion 2: What is marked on the above image?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q2 is: A. free fluid, B. lymph node C., inflamed appendix with target sign
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q2 is: A. free fluid, B. lymph node C., inflamed appendix with target sign
-
Question 3 of 4
3. Question
Discussion:
Acute appendicitis is one of the most common causes of acute abdominal pain in children. The pathophysiology typically involves luminal obstruction, most commonly due to lymphoid hyperplasia in children, leading to increased intraluminal pressure, ischemia, and subsequent inflammation of the appendix. If untreated, this can progress to gangrene, perforation, and generalized peritonitis. Ultrasound is often performed as the first-line imaging in patients where there is a suspicion of appendicitis, particularly in children, due to its non-invasive nature and lack of ionizing radiation. Classic ultrasound findings include a non-compressible, blind-ending tubular structure in the RLQ with a diameter exceeding 6 mm. Additional findings, such as periappendicular fluid, increased echogenicity of the surrounding fat, or the presence of an appendicolith, can further support the diagnosis. In our case the lack of widespread fluid or systemic symptoms ruled out diffuse inflammatory processes, helping to guide prompt management.
Radiologists must differentiate appendicitis from other conditions such as mesenteric adenitis or ovarian torsion, which can present similarly. Careful interpretation of ultrasound findings, combined with clinical history, ensures accurate diagnosis and timely management, particularly when complications like abscess or perforation are suspected.
This case underlines the importance of a systematic ultrasound evaluation in the right lower quadrant, understanding key anatomical landmarks, and recognizing the sonographic signs of appendicitis. Radiologists must also know when further imaging, such as CT or MRI, is needed in ambiguous cases, particularly when non-operative management is considered.
Question 3: When performing an ultrasound examination for suspected appendicitis in a pediatric patient, what is the most important factor in choosing the appropriate transducer?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q3 is: The frequency of the transducer, with higher frequencies providing better resolution for superficial structures like the appendix.
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q3 is: The frequency of the transducer, with higher frequencies providing better resolution for superficial structures like the appendix.
-
Question 4 of 4
4. Question
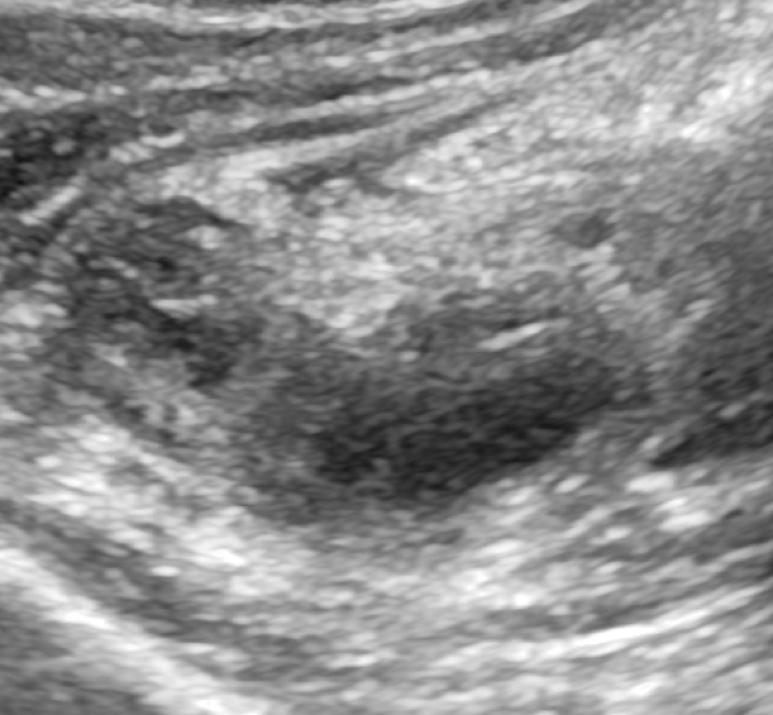
Image 4: Image from C1-6 transducer (GE Ultrasound, 1-6 MHz). The appendix is faintly visible
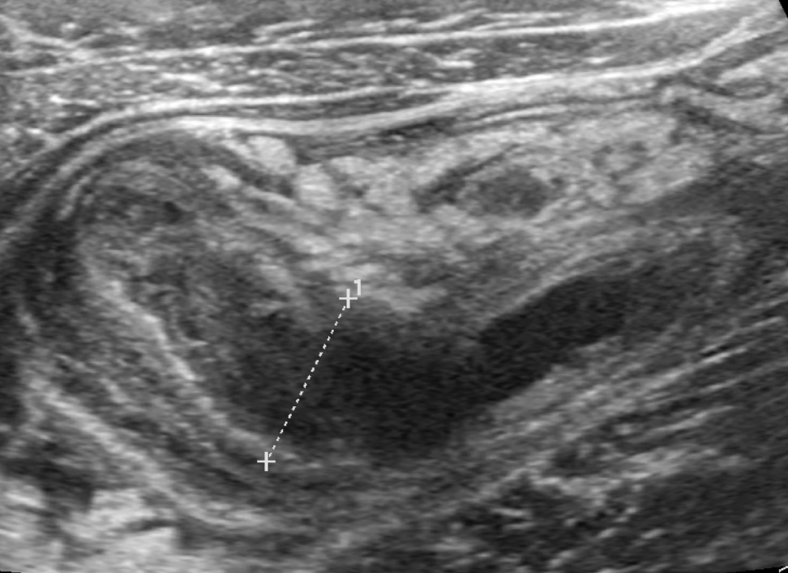
Image 5: Image from ML 6-15 transducer (GE Ultrasound, 6-15 MHz). The appendix is clearly visible
Additional discussion
When selecting a transducer for pediatric ultrasound, particularly for visualizing structures like the appendix, the frequency of the transducer is a critical factor. Higher-frequency transducers provide better resolution for superficial structures, such as the appendix, allowing clearer visualization of inflammation, fluid, and other diagnostic features. While lower-frequency transducers are better suited for imaging deeper structures, they may lack the resolution needed to accurately assess smaller or superficial anatomy, making them less ideal for pediatric purposes.
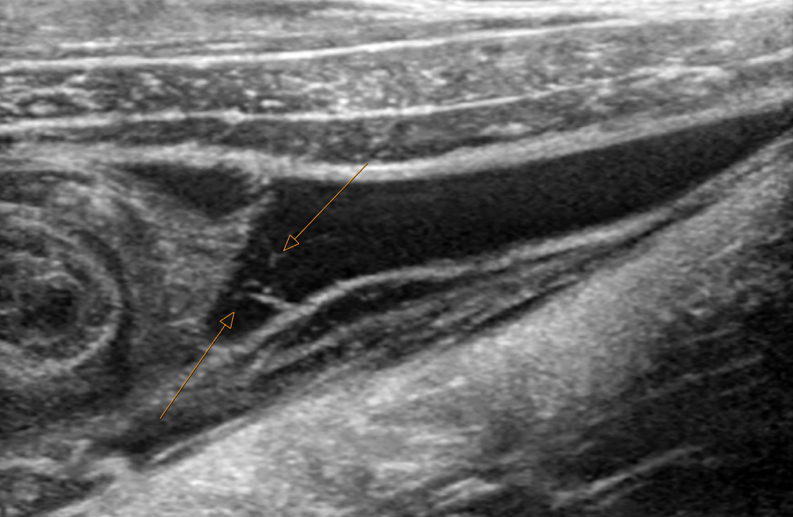
Image 6: Periappendicular fluid with septa and debris (arrow)
Question 4: What is the most likely explanation for the fluid collection around the appendix in this patient with suspected appendicitis?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q4 is: Localized ruptured appendicitis with abscess formation
Additional Discussion:
Fluid around the appendix in the setting of acute appendicitis is due to localized inflammation, which can lead to a reactive effusion or early abscess formation. Generalized peritonitis would involve more diffuse fluid accumulation, while omental infarction and retroperitoneal hematoma are less likely. The presence of localized fluid near the appendix strongly indicates a local inflammatory response. In our case a perforated appendix and periappendicular abscess was seen intraoperatively.
Conclusion
This case illustrates the essential role of ultrasound in diagnosing acute appendicitis in pediatric patients. The use of high-frequency transducers significantly improves image quality for visualizing superficial structures like the appendix. Key ultrasound findings, such as a non-compressible, enlarged appendix and peri-appendiceal fluid, allow for a confident diagnosis even in the absence of an appendicolith. Radiologists must also consider other potential causes of right lower quadrant pain and ensure careful interpretation of imaging within the clinical context. Choosing the appropriate transducer and recognizing early complications, such as abscess formation, are crucial for guiding timely and effective patient management.
Conflicts of interest
The authors declare no conflict of interest.
References
- Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 6th ed. Philadelphia: Elsevier; 2024.
- Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia: Elsevier; 2025.
- Hagen-Ansert SL. Textbook of Diagnostic Sonography. 9th ed. St. Louis: Elsevier; 2023.
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q4 is: Localized ruptured appendicitis with abscess formation
Additional Discussion:
Fluid around the appendix in the setting of acute appendicitis is due to localized inflammation, which can lead to a reactive effusion or early abscess formation. Generalized peritonitis would involve more diffuse fluid accumulation, while omental infarction and retroperitoneal hematoma are less likely. The presence of localized fluid near the appendix strongly indicates a local inflammatory response. In our case a perforated appendix and periappendicular abscess was seen intraoperatively.
Conclusion
This case illustrates the essential role of ultrasound in diagnosing acute appendicitis in pediatric patients. The use of high-frequency transducers significantly improves image quality for visualizing superficial structures like the appendix. Key ultrasound findings, such as a non-compressible, enlarged appendix and peri-appendiceal fluid, allow for a confident diagnosis even in the absence of an appendicolith. Radiologists must also consider other potential causes of right lower quadrant pain and ensure careful interpretation of imaging within the clinical context. Choosing the appropriate transducer and recognizing early complications, such as abscess formation, are crucial for guiding timely and effective patient management.
Conflicts of interest
The authors declare no conflict of interest.
References
- Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 6th ed. Philadelphia: Elsevier; 2024.
- Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia: Elsevier; 2025.
- Hagen-Ansert SL. Textbook of Diagnostic Sonography. 9th ed. St. Louis: Elsevier; 2023.