

Case of the month February 2025: Acute leg pain in a sedentary man
February 3, 2025
Case of the month April 2025: Palpable mass
April 1, 2025
Alexander Berkfors 1 and Samir Jawad 1
1 Department of Radiology, Rigshospitalet, Copenhagen University Hospital, Denmark
* Correspondence: alexander.skovbaek.berkfors@regionh.dk
Clinical history
An otherwise healthy 7-year-old boy was referred to the pediatric department due to sudden and severe, right-sided groin pain, with onset 2 hours prior to arrival. The pain was accompanied by the appearance of a lump in the right groin. There were no other gastrointestinal or urogenital symptoms.
Physical examination revealed a tender 4-5 cm long and 2-3 cm wide palpable mass in the right inguinal region, extending into the scrotum. Upon examination, the testis was palpable on the left side but not on the right side. Apart from these findings, the clinical examination was unremarkable.
An ultrasound examination was performed.
Images

Video 1: Dynamic scan on the right side from the inguinal region to the scrotum, cranial to caudal direction, in the axial plane.
Quiz-summary
0 of 2 questions completed
Questions:
- 1
- 2
Information
View the March Case below, answer the question and then click check >
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 2 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
- 1
- 2
- Answered
- Review
-
Question 1 of 2
1. Question
Question 1: What is the most likely cause of the patient’s pain?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q1 is: Irreducible inguinal hernia
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q1 is: Irreducible inguinal hernia
-
Question 2 of 2
2. Question
Discussion / Ultrasound description
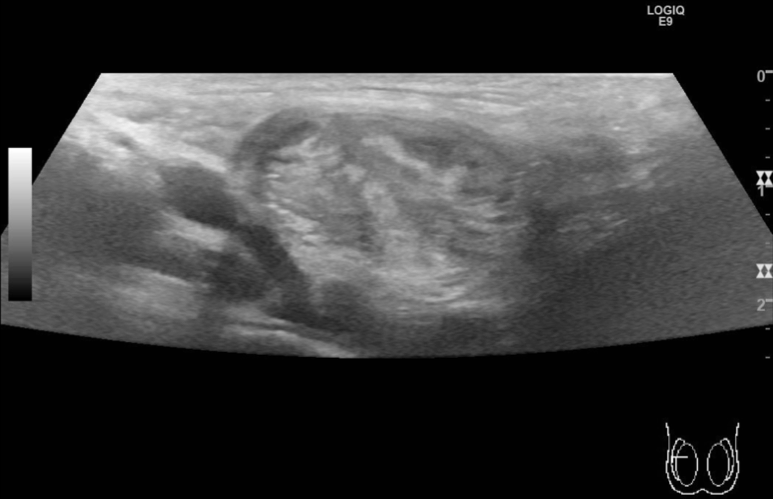
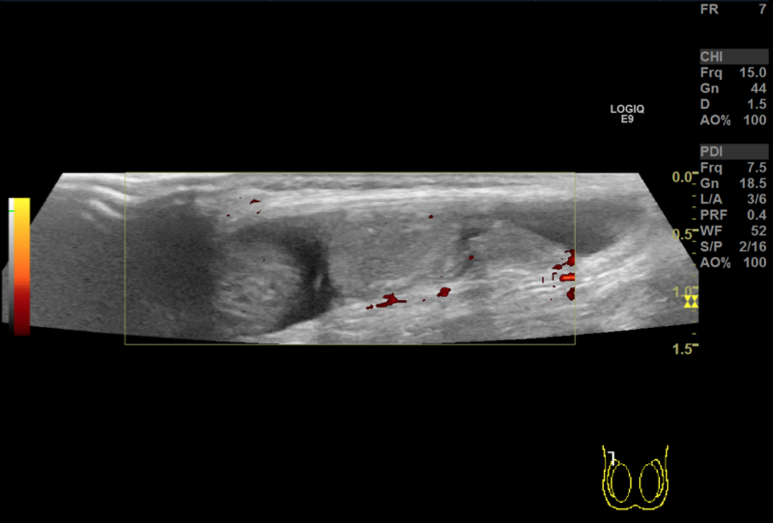
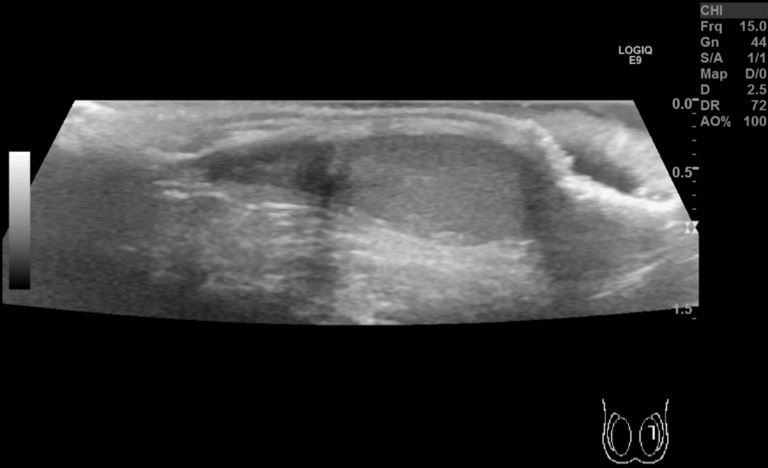
Ultrasound reveals a right sided inguinoscrotal hernia with a single loop of bowel occupying almost the entire inguinal canal, extending just cranially to the right testis which is located in the caudal part of the scrotum. The herniated bowel has a thick and edematous wall but acceptable flow visualized with Doppler. Within the bowel, fecal matter can be seen. A large right-sided hydrocele is also noted – likely reactive. There is very sparse color Doppler flow in the right testis, which also has slightly reduced echogenicity.
Additional Images
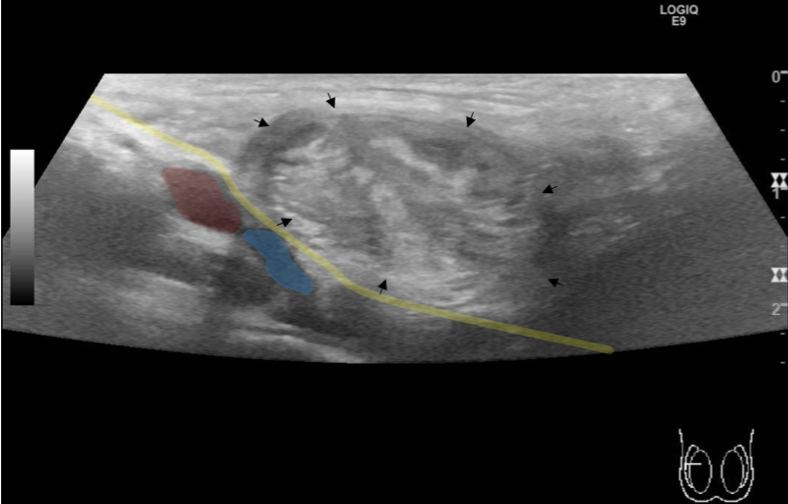
Image 4: (Image # 1 (with annotations): Yellow line marks the anatomical location of the inguinal ligament representing the floor of the inguinal canal. Above the inguinal ligament, black arrows mark an inguinal hernia, which contain a single bowel loop. Further annotations: femoral artery (red area) and femoral vein (blue area).
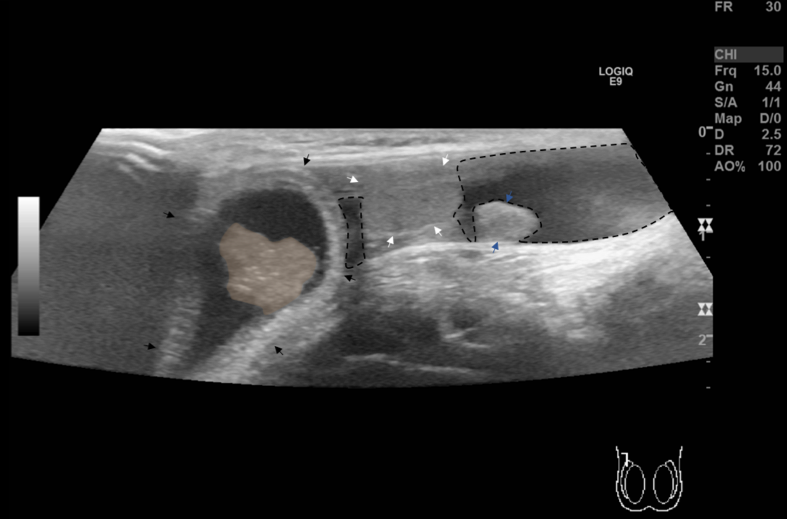
Image 5 ( Image # 2 with annotations): The black arrows mark an inguinal hernia containing a single loop of bowel occupying almost the entire inguinal canal – within the bowel, fecal matter can be seen (the brown area). The white arrows mark the testes. The blue arrows mark the tail of the epididymis. The dashed line outlines areas with hydrocele.
Question 2: What is the most likely cause of the testicular hypoperfusion?
Correct
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q2 is: Hypoperfusion secondary to inguinal hernia
Additional discussion
In light of the finding of an incarcerated inguinal hernia, this is the most likely cause of the testicular hypoperfusion. Especially since symptoms resolved after mild sedation and manual hernia reduction.
Discussion
Inguinal hernias, the most common hernia and far more likely in men, arise when intraabdominal or extraperitoneal organs protrude into the inguinal canal, either directly or indirectly. [1]Direct inguinal hernias usually develop gradually over time, and are more commonly seen in adults. They are caused by a weak spot (i.e. thinning) in the fascia transversalis, and develop as a consequence of physical strain. [2]
Indirect hernias predominately arise in children. They occur because of a patent processus vaginalis which is formed in the 8th gestational week, in boys by the descending testes into the scrotum, and in girls from the migration of the ligamentum rotundum. The processus vaginalis usually closes within the first year of life, but will remain patent in 12-19% of children into adulthood. Individuals with a patent processus vaginalis do not necessarily develop a hernia, but are at higher risk. The indirect hernia (as opposed to the direct hernia) is far more likely to cause bowel obstruction, since the hernia may descend all the way into the inguinal canal, which is narrow and long, and may cause strangulation of the tissue. If untreated, it may lead to necrosis within a couple of hours. [3]
With a clinical history of a sudden inguinal bulge and accompanying pain in a child, the most likely diagnosis is an indirect inguinal hernia, howerever differential diagnoses to consider are lymphadenopathy, abscess, hematoma, epidydimitis, hydrocele, femoral hernia, tersticular torsion, cryptorchidism with/without torsion, and amyand hernia. [1]
An inguinal hernia is primarily a clinical diagnosis, but in cases of doubt, ultrasound may guide the clinician in confirming the diagnosis or ruling out potential differential diagnoses. Be aware that a patient without complaints with an incidental finding of a patent processus vaginalis on ultrasound, does not require surgical management nor a consultation [4].
The management of a pediatric inguinal hernia, as in this case, is first and foremost done with manual hernia reduction. If manual hernia reduction fails, the treatment is emergency surgery. If manual hernia reduction is succesful, elective surgery is usually scheduled. (5)
Conclusion
Ultrasound is a readily available tool to evaluate scrotal emergencies in pediatric and adult patients.
Conflicts of Interest:
“The authors declare no conflict of interest.”
References
- Hammoud, M., & Gerken, J. (2023, August 8). Inguinal Hernia. StatPearls – NCBI Bookshelf.
- Morrison, Z., Kashyap, S., & Nirujogi, V. L. (2023, August 28). Adult Inguinal Hernia. StatPearls – NCBI Bookshelf.
- Öberg, S., Andresen, K., & Rosenberg, J. (2017). Etiology of Inguinal Hernias: A Comprehensive Review. Frontiers in Surgery, 4.
- Jamadar, D. A., Jacobson, J. A., Morag, Y., Girish, G., Ebrahim, F., Gest, T., & Franz, M. (2006). Sonography of Inguinal Region Hernias. American Journal of Roentgenology, 187(1), 185–190.
- Christoffer Skov Olesen, Kristoffer Andresen, Stina Öberg & Jacob Rosenberg. Lyskebrok hos børn. Ugeskrift for læger. 2019.
Incorrect
CORRECT ANSWER EXPLAINED BELOW Correct answer to Q2 is: Hypoperfusion secondary to inguinal hernia
Additional discussion
In light of the finding of an incarcerated inguinal hernia, this is the most likely cause of the testicular hypoperfusion. Especially since symptoms resolved after mild sedation and manual hernia reduction.
Discussion
Inguinal hernias, the most common hernia and far more likely in men, arise when intraabdominal or extraperitoneal organs protrude into the inguinal canal, either directly or indirectly. [1]Direct inguinal hernias usually develop gradually over time, and are more commonly seen in adults. They are caused by a weak spot (i.e. thinning) in the fascia transversalis, and develop as a consequence of physical strain. [2]
Indirect hernias predominately arise in children. They occur because of a patent processus vaginalis which is formed in the 8th gestational week, in boys by the descending testes into the scrotum, and in girls from the migration of the ligamentum rotundum. The processus vaginalis usually closes within the first year of life, but will remain patent in 12-19% of children into adulthood. Individuals with a patent processus vaginalis do not necessarily develop a hernia, but are at higher risk. The indirect hernia (as opposed to the direct hernia) is far more likely to cause bowel obstruction, since the hernia may descend all the way into the inguinal canal, which is narrow and long, and may cause strangulation of the tissue. If untreated, it may lead to necrosis within a couple of hours. [3]
With a clinical history of a sudden inguinal bulge and accompanying pain in a child, the most likely diagnosis is an indirect inguinal hernia, howerever differential diagnoses to consider are lymphadenopathy, abscess, hematoma, epidydimitis, hydrocele, femoral hernia, tersticular torsion, cryptorchidism with/without torsion, and amyand hernia. [1]
An inguinal hernia is primarily a clinical diagnosis, but in cases of doubt, ultrasound may guide the clinician in confirming the diagnosis or ruling out potential differential diagnoses. Be aware that a patient without complaints with an incidental finding of a patent processus vaginalis on ultrasound, does not require surgical management nor a consultation [4].
The management of a pediatric inguinal hernia, as in this case, is first and foremost done with manual hernia reduction. If manual hernia reduction fails, the treatment is emergency surgery. If manual hernia reduction is succesful, elective surgery is usually scheduled. (5)
Conclusion
Ultrasound is a readily available tool to evaluate scrotal emergencies in pediatric and adult patients.
Conflicts of Interest:
“The authors declare no conflict of interest.”
References
- Hammoud, M., & Gerken, J. (2023, August 8). Inguinal Hernia. StatPearls – NCBI Bookshelf.
- Morrison, Z., Kashyap, S., & Nirujogi, V. L. (2023, August 28). Adult Inguinal Hernia. StatPearls – NCBI Bookshelf.
- Öberg, S., Andresen, K., & Rosenberg, J. (2017). Etiology of Inguinal Hernias: A Comprehensive Review. Frontiers in Surgery, 4.
- Jamadar, D. A., Jacobson, J. A., Morag, Y., Girish, G., Ebrahim, F., Gest, T., & Franz, M. (2006). Sonography of Inguinal Region Hernias. American Journal of Roentgenology, 187(1), 185–190.
- Christoffer Skov Olesen, Kristoffer Andresen, Stina Öberg & Jacob Rosenberg. Lyskebrok hos børn. Ugeskrift for læger. 2019.