Quiz-summary
0 of 2 questions completed
Questions:
- 1
- 2
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 2 questions answered correctly
Time has elapsed
Categories
- Not categorized 0%
-
That is Case 03 completed – to move on to Case 04 ~ click here
- 1
- 2
- Answered
- Review
-
Question 1 of 2
1. Question
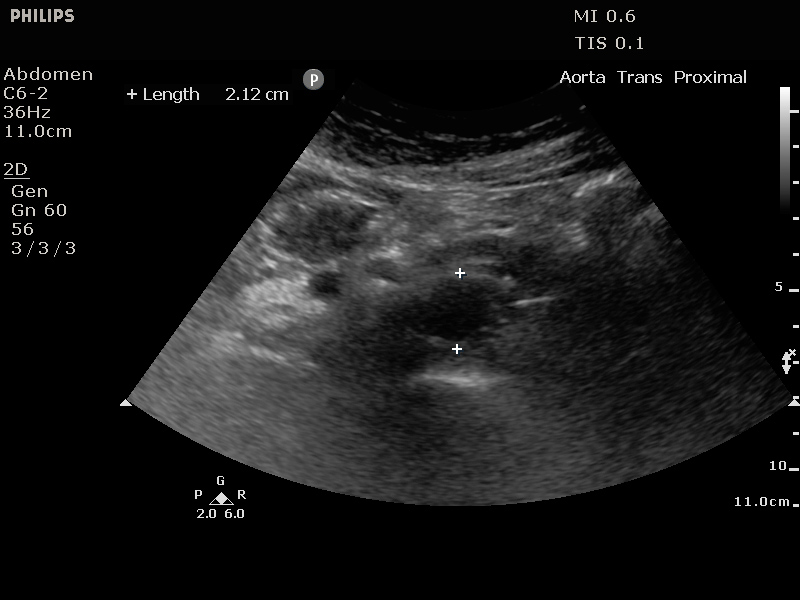
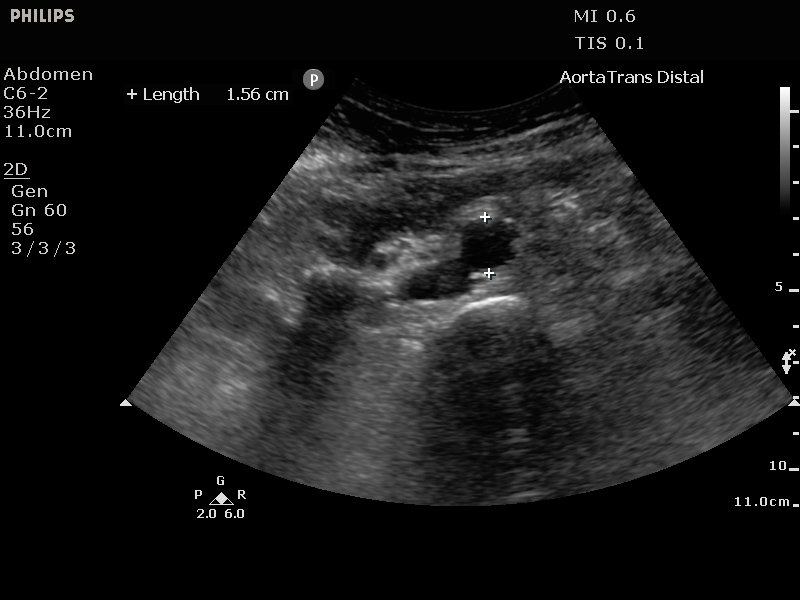
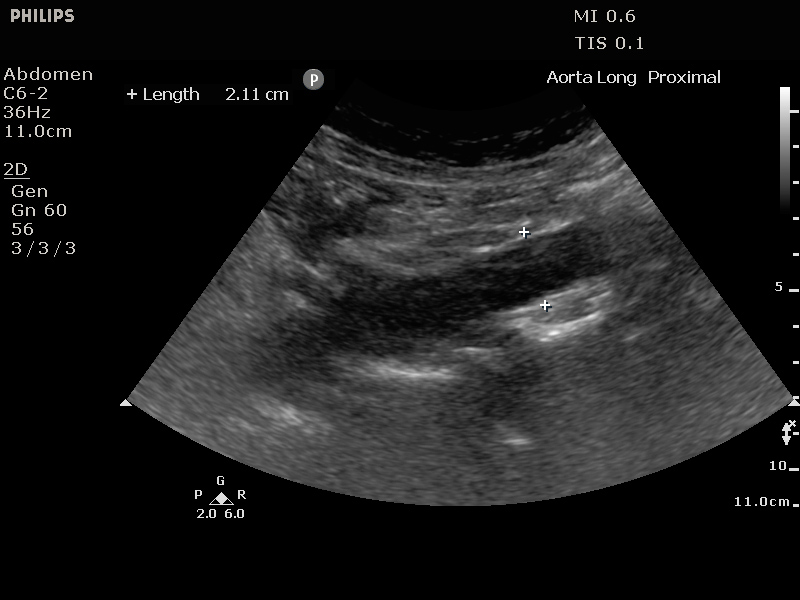
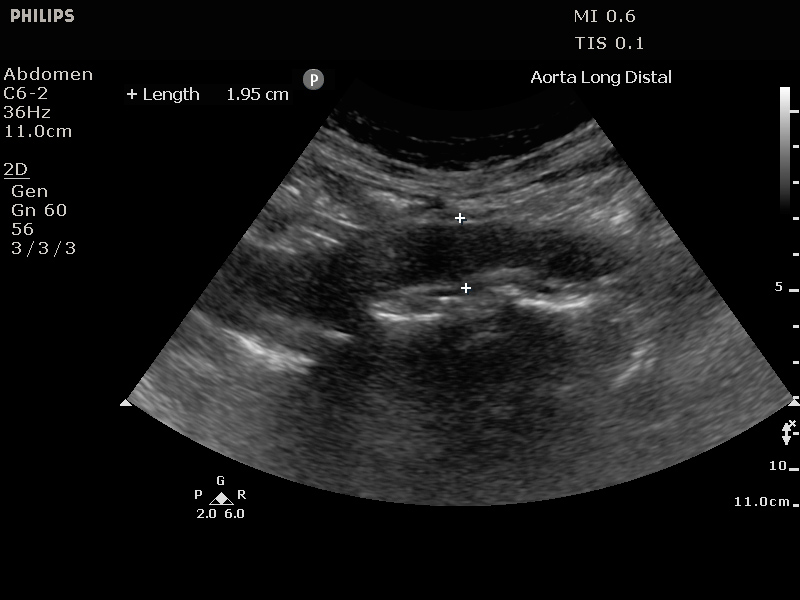
Clinical Description:
62 yr old previously well man with increasing abdominal pain radiating through to back and down left iliac fossa and nausea presents to a peripheral hospital with on call (but not on site) CT. O/E Restless, distressed, BP 150/80 otherwise normal obs.
Is there an abdominal aortic aneurysm?
Correct
Although the images could be improved by adjusting the depth and gain, there is no aortic aneurysm.
Incorrect
-
Question 2 of 2
2. Question
Clinical Description:
62 yr old previously well man with increasing abdominal pain radiating through to back and down left iliac fossa and nausea presents to a peripheral hospital with on call (but not on site) CT. O/E Restless, distressed, BP 150/80 otherwise normal obs.
What is an appropriate management for this patient?
Correct
AAA is an important differential for renal colic. History (e.g. previous Hx of stones) and examination (?pulsatile mass) can help, but ultrasound can usually rapidly exclude the diagnosis with more certainty. Other differentials for abdominal pain should be considered but if the clinical picture is typical of renal colic (flank pain, haematuria, etc.) and no ‘red flags’ (fever, single kidney, worsening renal function) then CT KUB can be arranged non-urgently or omitted (typical picture in patient with history of recurrent stones) Local protocols vary on which renal colic patients may not require any imaging.
Incorrect